This post is an answer to the Case – A 62-year-old Man with Periocular Purpura
Histological examination showed accumulation of amorphous eosinophilic masses below the epidermis in the papillary and upper reticular dermis, around sweat glands and hair follicles. Staining for thioflavine T showed yellow-green immunofluorescence. Congo red staining showed apple-green birefringence on polarised light microscopy, indicating amyloid deposits.

Serum protein electrophoresis showed the presence of a monoclonal (M) protein. Immunofixation of both serum and urine determined its type: IgA-λ-type Bence-Jones protein. Bone-marrow examination was diagnostic for myeloma.
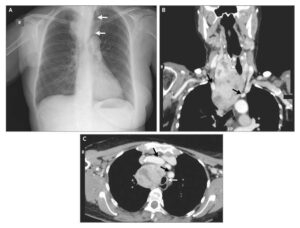
Radiography showed small osteolysis of the head and cervical spine. Further investigations showed bilateral carpal tunnel syndrome and cardiac involvement. The diagnosis of systemic AL-amyloidosis was made from the combination of clinical findings, the presence of amyloid deposits in skin biopsy sample, and the plasma cell dyscrasia.
Treatment with bortezomib, cyclophosphamide, and dexamethasone was given. Autologous haemopoietic cell transplantation is planned.
Systemic AL-amyloidosis is a rare and severe disease. Bruising purpura around the eyelids combined with yellow waxy papules are typical clinical signs suspicious for systemic AL-amyloidosis. This disease occurs in patients with plasma cell dyscrasia, in particular multiple myeloma.
Amyloid is composed of a fibrillar component (immunoglobulin light chain material derived from the abnormal paraprotein) and a nonfibrillar protein termed amyloid P component. It deposits in extracellular tissue of several organs (skin, kidney, heart, liver, and peripheral nerve system). The prognosis depends on the number and severity of internal organ involvement and haematological response to treatment.
SIMILAR CASE: Periorbital Purpura