This post is an answer to the Case – 33-year-old Man With Shortness of Breath
Findings
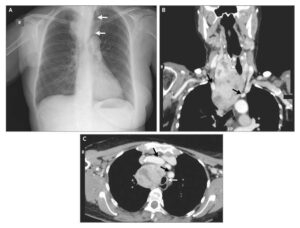
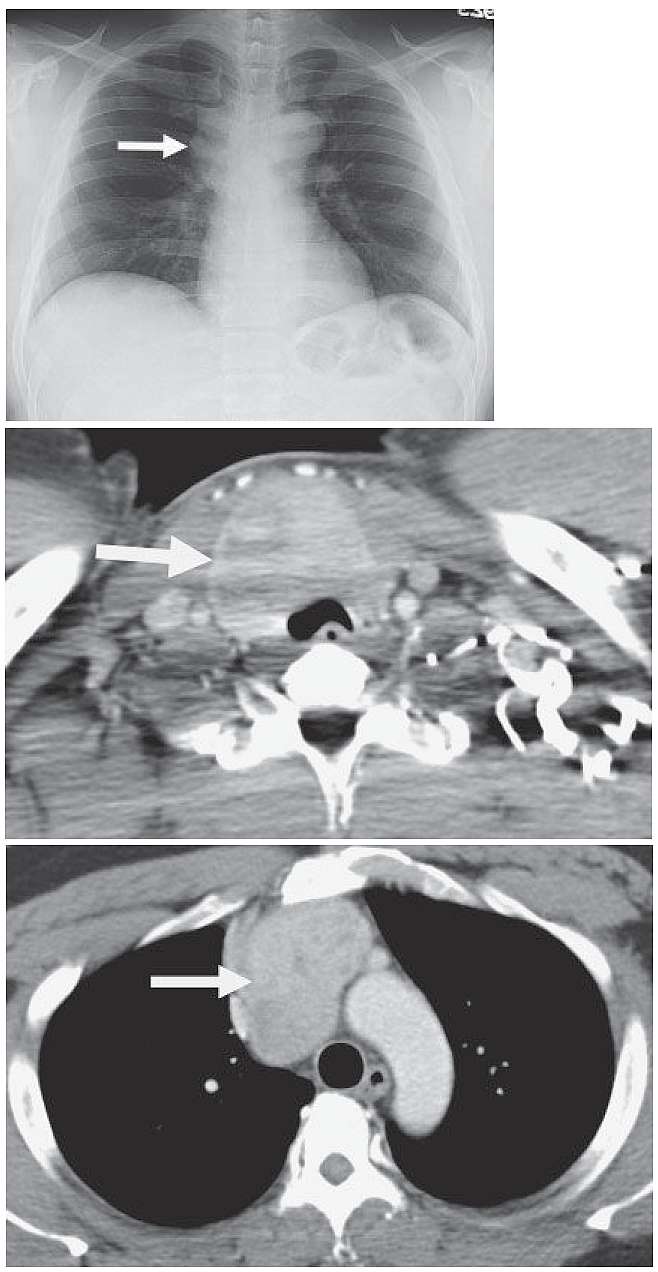
- Frontal chest radiograph demonstrates a right paratracheal mass (arrow in first image), which on the lateral view displaces the trachea posteriorly, indicating that the mass lies in either the right paratracheal space or anterior mediastinum. Note that the superior edge of the mass is not well seen.
- Subsequent CT demonstrates a heterogeneously enhancing mass (arrows in second and third image) extending from an enlarged thyroid into the anterior mediastinum. The mass also exerts mass effect on the anterior tracheal wall near the thoracic inlet.
Differential Diagnosis
Based on the chest radiograph, the differential diagnosis would be headed by an anterior mediastinal mass, given that the center of the lesion lies anterior to the trachea. The differential diagnosis would include germ cell tumor and lymphoma, based on the patient’s young age. Occasionally, thymoma and goiter may present in younger adults. The CT would be diagnostic of goiter.
Teaching Points
- Substernal goiters are common, approaching 15% , depending on how the term “substernal” is defined. There is a low but significant risk of malignancy, ranging from 3 % to 21 % .
- While often symptomatic, large goiters can present with airway compromise or due to vascular compression.
- Approximately 1 % of goiters are considered primary retrosternal lesions with no communication with the cervical thyroid. Secondary retrosternal goiters that communicate with the cervical thyroid may display a cervicothoracic sign (extension of the mass above the thoracic inlet) in which the superior margin is ill defined due to blending with neck soft tissues, unlike the case of a posterior mediastinal mass, which is nicely outlined by the apical portions of the lung.
Management
Surgical resection is the treatment of choice. In experienced hands, almost all lesions can be resected via a cervical approach, avoiding median sternotomy.
SIMILAR CASES:
Further Reading
Cohen, J.P. (2009), Substernal goiters and sternotomy. The Laryngoscope, 119: 683-688. https://doi.org/10.1002/lary.20102