This post is an answer to the Case – Patient with Severe Pneumonia
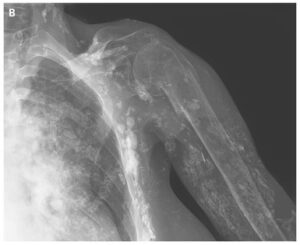
The chest radiography showed a radiopaque left hemithorax with right shift of the mediastinum. Double-contrast barium enema demonstrated the presence of large part of the intestine inside the left hemithorax (image below).

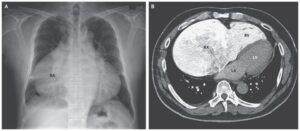
CT examination revealed complete occupation of the left hemithorax by abdominal organs. Namely, the left hemithorax contained the spleen, small and large intestine and a large quantity of mesenteric fat. The small and large intestine lied in the periphery of the thoracic cavity while its central part was occupied by mesenteric fat.
CT also revealed a hypoplastic left lung, the presence of left pulmonary artery and a blind-ended left main bronchus. Finally, the CT examination demonstrated a defect in the left hemidiaphragm, which caused the intrathoracic displacement of the abdominal organs.
Multi-planar reconstructions (MPR) and Volume Rendering Techniques (VRT) were performed to better delineate the findings.
Differential Diagnosis
- Pulmonary hypoplasia caused by a large congenital diaphragmatic hernia.
- Cystic adenomatoid malformation
- Pulmonary agenesis
- Pulmonary aplasia
- Pulmonary hypoplasia
- Congenital diaphragmatic hernia
Discussion about Pulmonary hypoplasia (PH)
Pulmonary hypoplasia (PH) is characterized by underdevelopment of the lung which is caused by any situation that limits the space of the thoracic cavity available for lung growth. The longer the underlying cause exists and the more intense it is, the more hypoplastic the lung will be. As in our case, a congenital diaphragmatic hernia is one of the most common causes of PH as the defect of the hemidiaphragm allows the abdominal organs to move into the thorax, thus compressing the developing lung.
Other intrathoracic causes of lung hypoplasia include sequestration, mediastinal masses, complete absence of the diaphragm and a large pleural effusion. Other causes include decreased pulmonary blood supply and extrathoracic diseases like oligohydramnios [2, 3]. Pulmonary hypoplasia may also be primary with a very low frequency (0.8-1.6 per 10000 births) [4].
Clinical presentation of PH comprises early respiratory distress after birth, cyanosis, tachypnoea, hypoxia with hypercapnea and acidosis. PH can be complicated by pneumothorax or pulmonary hypertension.
Chest radiography of a patient with PH will show decreased radiolucency in the affected lung (more often the right). The mediastinum may be displaced towards the affected side due to compensatory ventilation of the normal lung and in some cases congenital bronchiectasis can be seen. On lateral chest radiography, hyperclarity may be seen behind the sternum due to herniation of the normal lung. Prenatal diagnosis with US is difficult but can be more easily done with MRI where the volume of the two lungs can be measured and the hypoplastic lung usually has lower signal intensity than normal [3, 5].
The majority of patients with PH die but there are also patients who survived and were diagnosed with imaging [4]. When surgery is planned, CT is the imaging modality of choice for preoperative planning as it describes better the anatomic extent of pathology [6]. Recent papers report that early fetoscopic tracheal occlusion increases the survival rate of infants with severe pulmonary hypoplasia and congenital diaphragmatic hernia [7].
References
- Schneider P, Schwalbe E. (1912) Die morphologie der missbildungen des menschen und der thiere. Jena: Fischer 3:812-822.
- Berrocal T, Madrid C, Novo S, Gutierrez J, Arjonilla A, Gomez-Leon N. (2004) Congenital anomalies of the tracheobronchial tree, lung and mediastinum: embryology, radiology and pathology. Radiographics 24(1):e17. (PMID: 14610245)
- Garcia-Pena P, Coma A, Enriquez G. (2013) Congenital lung malformations: radiological findings and clues for differential diagnosis. Acta Radiol Feb 23 [Epub ahead of print]. (PMID: 23436824)
- Lauria MR, Gonik B, Romero R. (1995) Pulmonary hypoplasia: pathogenesis, diagnosis and antenatal prediction. Obstet Gynecol 86(3):466-75. (PMID: 7651663)
- Çay A, Sarihan H. (2000) Congenital malformation of the lung. J Cardiovasc Surg 41:507-510. (PMID: 10952352)
- Mata JM, Caseres J, Lucaya J, Garcia-Conesa JA. (1990) CT of congenital malformations of the lung. Radiographics 10(4):651-74. (PMID: 2377765)
- Ruano R, Peiro JL, da Silva MM, Campos JA, Carreras E, Tannuri U, et al. (2013) Early fetoscopic tracheal occlusion for extremely severe pulmonary hypoplasia in isolated congenital diaphragmatic hernia: preliminary results. Ultrasound Obstet Gynecol 42(1):70-6. (PMID: 23349059)