
This post is an answer to the Case – Patient with Progressive Breathlessness
An urgent chest X-ray revealed a large left-sided pneumothorax with evidence of tension and a cystic structure in the left lower zone. A chest drain was inserted and a repeat chest X-ray was taken. The left lung had re-expanded but there was an opacity in the left costophrenic angle.
Clinically the patient improved and the chest drain was removed. Within 36 hours of removal the patient became symptomatic again and the chest X-ray was repeated. The pneumothorax had recurred and the left costophrenic angle opacity was still present.
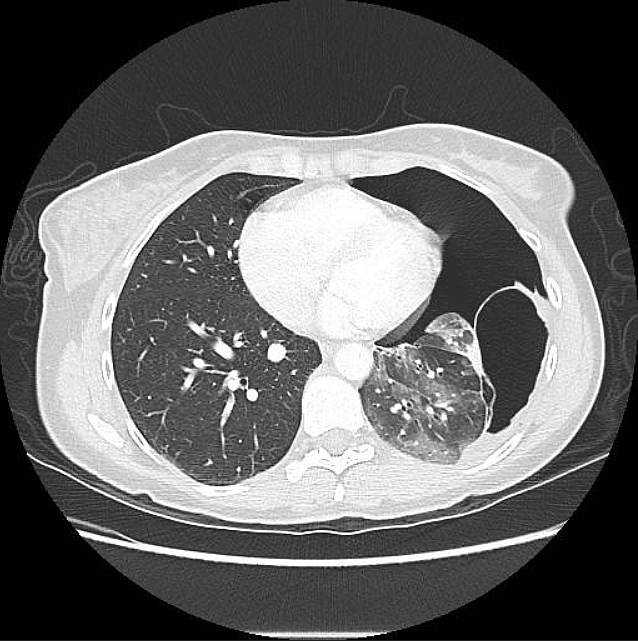
A contrast-enhanced CT of the thorax was then performed and revealed a moderately sized left-sided pneumothorax and a well-defined, thick-walled air-filled structure arising from the left lower lobe and adherent to the parietal pleura (image below).
After multi-disciplinary team discussion it was decided that excision was the best option to avoid repeated pneumothoraces and obtain histological diagnosis.
A video-assisted thorascopic excision was performed with no complication. Histology revealed epithelial cells entirely consistent with a bronchogenic cyst.
Discussion about Bronchogenic cysts
Background
Bronchogenic cysts are a congenital abnormality resulting from abnormal development of the tracheobronchial tube, they are part of the family of foregut duplication cysts, enteric cysts and neuroenteric cysts.
Cysts are most commonly located in the lung parenchyma or mediastinum and if they communicate with the bronchial tree they will be air filled or contain an air-fluid level. Their location depends on the embryological stage of development at which the anomaly occurs. Cysts that arise later are more peripheral [1].
Clinical perspective
Previously thought to be asymptomatic and innocent anomalies, recent studies have reported symptoms and complications from bronchogenic cysts and advise surgical excision even in cases without symptoms [2, 3, 4]. Complications from bronchogenic cysts are not uncommon (45%) [5] and include compression of adjacent structures, infection, haemoptysis and not uncommonly pneumothorax as in this case.
Imaging Perspective
Appearances on imaging vary depending on the contents of the cyst whether it be fluid, air or a combination of both. CT imaging findings are characteristically of a well-circumscribed round or ovoid solitary lesion with uniform fluid attenuation on CT [7] although the attenuation value can vary with the amount of proteinaceous content.
With the administration of IV contrast a non-enhancing or minimally enhancing thin wall is typically seen and the wall can calcify. Thick enhancing walls, septations, solid components and internal calcifications are not typically demonstrated [8].A definitive diagnosis of a bronchogenic cyst is made when respiratory epithelium is histologically present.
Outcome
Bronchogenic cysts are benign abnormalities and usually do not recur after excision. The prognosis after excision is excellent although incomplete excision can lead to recurrence and in some patients with pulmonary lesions lobectomy may be necessary [6]. This patient made a full recovery and was discharged by the cardiothoracic team.
References
- Aktogu S, Yuncu G (1996) Bronchogenic cysts: clinicopathological presentation and treatment. Eur Respir J 9: 2017-2021 (PMID: 8902460)
- St. Georges R, Deslauriers J, Duranceau A, et al. (1991) Clinical spectrum of bronchogenic cysts of the mediastinum and lung in the adult. Ann Thorac Surg 52: 6-13 (PMID: 2069465)
- Patel SR, Meeker DP, Biscottii CV, Kirby TJ, Rice TW. (1994) Presentations and management of bronchogenic cysts in the adult. Chest 106: 79-85
- Sirivella S, Ford WB, Zikria EA, Miller WH, Samadani SR, Sullivan ME. (1985) Foregut cysts of the mediastinum. Results in 20 consecutively treated cases. J Thorac Cardiovascu Surg 90:776-782. (PMID: 4058048)
- Sarper A, Ayten A, Golbasi I, Demircan A, Isin E (2003) Bronchogenic cyst. Texas heart institute journal 30(2):105-108 (PMID: 12809250)
- Suen HC, Mathisen DJ, Grillo HC. (1993) Surgical management and radiological characteristics of bronchogenic cysts. Ann Thorac Surg 55: 476-81 (PMID: 8431062)
- Lee EY, Boiselle PM, Cleveland RH (2008) Multidetector CT Evaluation of Congenital Lung Anomalies. Radiology 247:632-648 (PMID: 18487532)
- Williams HJ, Johnson KJ (2002) Imaging of congenital cystic lung lesions. Paediatr Respir Rev 3: 120-127 (PMID: 12297058)
