
This article is an answer to the Case – 25-year-old Woman with Abrupt Decrease in Oxygen Saturations
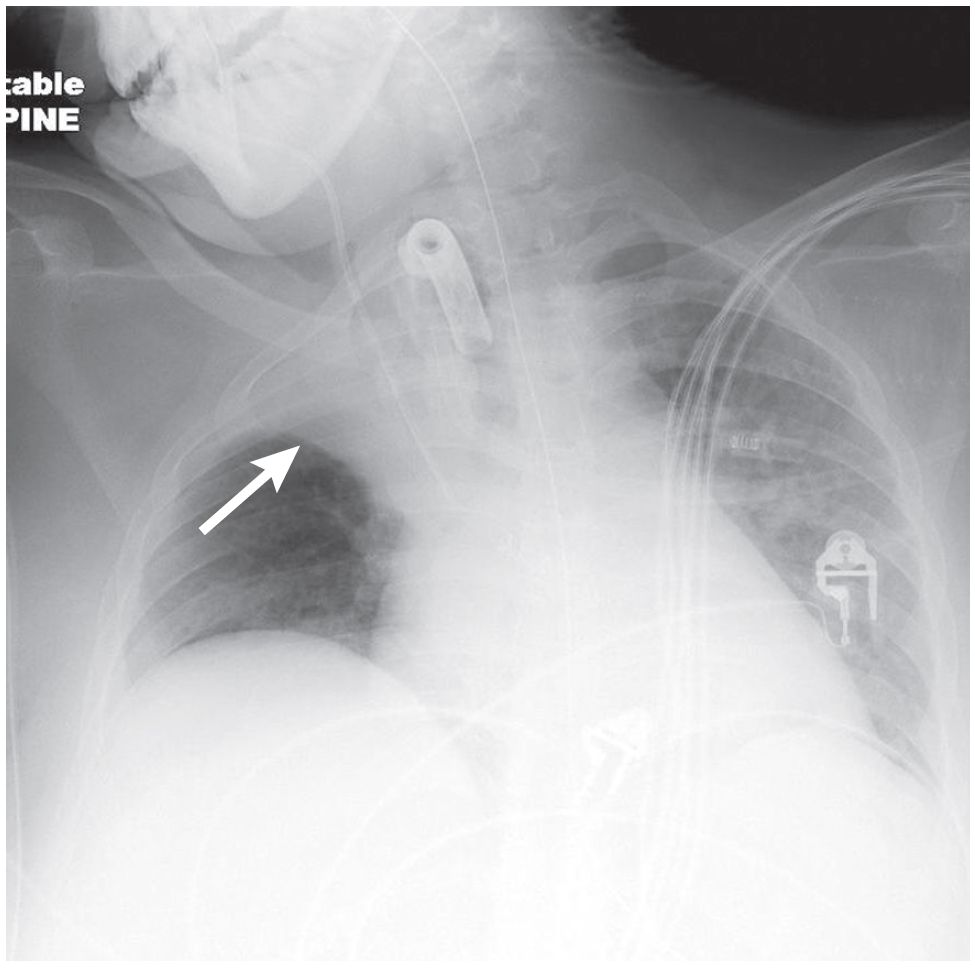
AP chest radiograph demonstrates opacification of the upper one-third of the right hemithorax without air bronchograms. The horizontal fissure (arrow) is displaced cephalad. Various life support tubes and lines are appropriately positioned. Free air beneath the left diaphragm is related to the concurrent recent PEG placement.
Diagnosis
Right Upper Lobe Atelectasis (Resorption); Endobronchial Mucus Plug
Differential Diagnosis
- Acute Lobar Collapse of Other Etiologies
- Aspirated or Dislodged Foreign Body (e.g., tooth, dental amalgam)
- Aspirated Peri-operative Blood/Endobronchial Clot
Clinical Findings
Complete lobar collapse may occur in 18–24 hours while breathing room air. Because oxygen is absorbed 60 times more rapidly than nitrogen, resorption atelectasis is expedited when breathing 100% oxygen, and total collapse may then occur in less than 1 hour. Some studies even report this occurring in as little as 5 minutes.
These latter situations may occur in intubated acute trauma patients, ICU ventilator-dependent patients, and surgical patients in the operating room under general anesthesia. Confirmation of appropriate ET tube positioning is critical in such patients.
Etiology
Acute resorption atelectasis may occur in trauma victims with aspirated foreign bodies (e.g., teeth, tooth fragments, dental amalgam, tongue rings, windshield glass fragments, etc.) as well as patients with an acute bronchial fracture.
More insidious resorption atelectasis occurs with primary and secondary endobronchial neoplasms, airway strictures or stenosis (e.g., granulomatous diseases, Wegener granulomatosis), and exobronchial lesions that extrinsically compromise the bronchus over time, such as the bulky lymphadenopathy associated with sarcoidosis or lymphoma.
Imaging Findings
Radiography/MDCT
- Acute development of segmental, lobar, or total lung collapse
- Absent air bronchograms
- Identify cause of the obstruction
- Rapid re-expansion of affected lung following relief of obstruction when possible
Management
- Respiratory physiotherapy (chest wall percussion and vibration), bronchiolytics, postural drainage, and bronchodilators
- Bronchoscopy in selected cases
- Relief of obstructing medical device (e.g., malpositioned endotracheal tube) or foreign body where appropriate
- N-acetylcysteine aerosols
- Nebulized or direct tracheal application of DNase may reduce viscoelastic properties of purulent airway secretions, reducing the viscosity and allowing easier clearance
- Endobronchial laser and stents in complicated cases
Prognosis
- Lung returns to normal after relief of obstruction and resolution of post-obstructive pneumonia in uncomplicated cases
- Untreated or unrecognized resorption atelectasis stemming from endobronchial obstruction may be complicated by:
- Persistent obstruction/infection
- Bronchiectasis with recurrent infection and/or hemoptysis
- Fibrosis
Pearls
- In children, obstruction is often due to a mucus plug or aspirated foreign body.
- In young adults (<35 years), obstruction is often due to a mucus plug, foreign body, or benign neoplasm.
- In older adults, primary and secondary endobronchial neoplasms must be excluded.