Table of Contents
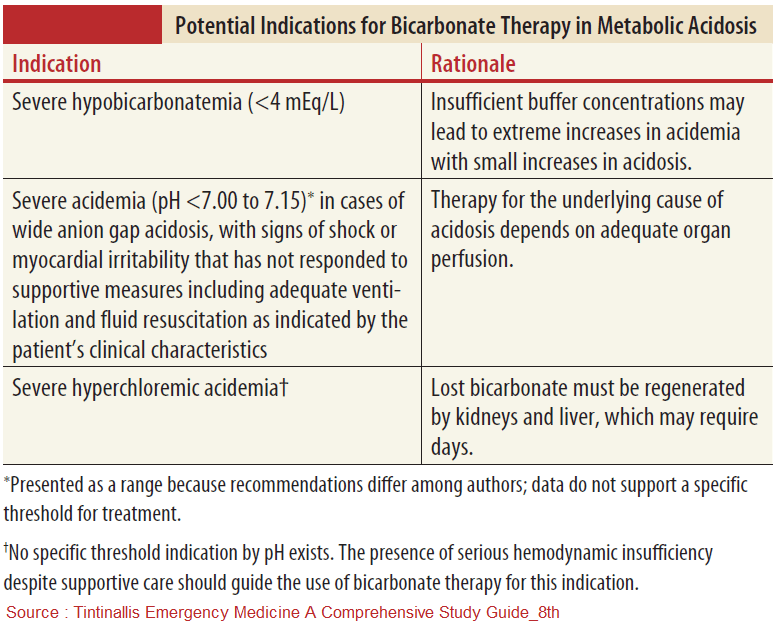
Sodium bicarbonate is an important antidote in the treatment of the critically ill poisoned patient. This contrasts with the general approach to acidosis due to other conditions, where sodium bicarbonate is rarely used and targeting the underlying illness (e.g., sepsis, diabetic ketoacidosis, acute renal failure) is the preferred strategy.
Sodium bicarbonate has a vital and specific role in a variety of poisonings, most notably those involving tricyclic antidepressants (TCAs) and salicylates.
Among the most important applications of sodium bicarbonate are:
- reversal of sodium channel blockade
- alteration of drug distribution and enhancement of elimination
- reversal of lifethreatening acidemia
Reversal of Sodium Channel Blockade
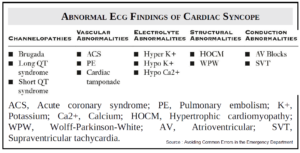
Blockade of the fast sodium channels may cause fatal cardiotoxic effects, manifested by conduction delays (QRS prolongation, right bundle branch block, wide complex tachycardias) and hypotension.
This toxidrome is well noted in poisonings by:
- tricyclic antidepressants (TCAs)
- type IA and IC antidysrhythmics (e.g., quinidine, procainamide, flecainide)
- diphenhydramine
- propoxyphene
- quinine
- carbamazepine
- cocaine
Sodium bicarbonate is an antidote that reverses the toxicity of sodium channel blockers by two mechanisms:
- It creates an alkaline environment that decreases the fraction of the ionized form of the drug available to bind and block the sodium channel
- it increases the number of sodium ions available to move through sodium channels.
The indications for sodium bicarbonate in sodium channel blocker toxicity are:
- QRS duration > 0.10 seconds
- ventricular dysrhythmias
- hypotension
Sodium bicarbonate does not effectively treat altered mental status or seizures associated with TCA poisoning; however, it may have utility in limiting further acidemia caused by seizures, which can exacerbate conduction disturbances and dysrhythmias.
Alteration of Drug Distribution and Enhancement of Elimination
Salicylate toxicity has a complex pathophysiology affecting multiple organ systems, and is discussed in greater depth in a separate chapter. Though there is no specific antidote for salicylate poisoning, the administration of sodium bicarbonate is a cornerstone of treatment.
Sodium bicarbonate acts both to decrease concentrations of salicylate in target tissues and to enhance elimination of salicylate in the urine via alkalinization.
Salicylate is a weak acid that converts to an ionized form as pH increases. Administration of sodium bicarbonate and subsequent ionization of the drug allows trapping of salicylate in the plasma compartment, as ionized molecules less readily cross cell membranes.
Importantly, this decreases binding of drug in the central nervous system (CNS), which causes the greatest morbidity and mortality related to salicylate poisoning. Furthermore, ionization of salicylate in an alkalinized urine environment augments the accumulation and subsequent elimination of salicylate in the urine.
Similar principles apply to poisoning by other weak acids, including phenobarbital, chlorpropamide, and chlorophenoxy herbicides.
Indications for sodium bicarbonate in salicylate poisoning include:
- symptoms or signs of systemic toxicity (i.e., CNS or pulmonary manifestations)
- significant metabolic acidosis
Some toxicologists also advocate for sodium bicarbonate administration in asymptomatic patients with a salicylate concentration >30 mg/dL.
Controversy exists regarding the indications for alkalinization, as excessive alkalemia, hypernatremia, fluid overload, hypokalemia, and hypocalcemia may result.
Management with endotracheal intubation and hyperventilation may be employed when necessary (using care to avoid worsening acidemia from respiratory acidosis), and hemodialysis may be required.
Reversal of Lifethreatening Acidemia
Toxic alcohol poisoning (e.g., ethylene glycol and methanol) can cause lifethreatening acidemia, associated with hemodynamic instability and end organ dysfunction.
Though definitive care must include administration of fomepizole or ethanol, and possibly hemodialysis, sodium bicarbonate may be an important temporizing measure to reverse severe acidemia.
It is recommended that sodium bicarbonate is administered when arterial pH is <7.30 in the setting of toxic alcohol poisoning. Additional benefits of sodium bicarbonate are the redistribution of toxic metabolites out of target tissues, and enhancement of urinary elimination.
Dosing of Sodium Bicarbonate
Dosing and administration of sodium bicarbonate is similar across multiple poisonings. A hypertonic sodium bicarbonate solution may be initiated as a 1- to 2-mEq/kg intravenous (IV) bolus over 1 to 2 minutes, followed by a continuous infusion.
The infusion is created through mixture of three 50 mL ampules of sodium bicarbonate (total of 150 mEq) into a 1-L bag of D5W, and run at approximately twice the maintenance rate. D5W is used because of its hypotonic properties. When combined with sodium bicarbonate, it creates an isotonic solution.
- Specifically for TCA poisoning, the initial IV bolus of sodium bicarbonate may be repeated every 5 minutes as needed to achieve narrowing of the QRS interval, and a blood pH of 7.50 to 7.55. Serial electrocardiograms (ECGs), arterial blood gases (ABGs) for pH monitoring, and reassessment of volume status are required as part of ongoing management. The infusion is usually discontinued when improvement in cardiotoxicity, hemodynamic indices, and mental status is achieved.
- For a goal of enhanced urinary elimination, as in salicylate poisoning, the infusion should be titrated to a goal urinary pH 7.5 to 8.0 and urine output of 3 to 5 mL/kg/h. ABGs should be followed to ensure serum pH does not exceed 7.55. To ensure successful alkalinization of urine, IV potassium supplementation (through addition of 20 to 40 mEq/L of fluid) may be necessary.
Key Points
- Though less applicable for the general critically ill patient with metabolic acidosis, sodium bicarbonate has a vital and specific role as an antidote in the poisoned patient.
- Sodium bicarbonate is a specific reversal agent in cases of poisoning from sodium channel blockers (i.e., TCA and type I antidysrhythmics).
- In salicylate toxicity, sodium bicarbonate favorably redistributes the drug out of vulnerable target tissues, and enhances urinary elimination.
- Sodium bicarbonate can temporize the severe and harmful metabolic acidosis seen in poisoning by toxic alcohols and is used concurrently with definitive care measures.
- Sodium bicarbonate is administered as a 1- to 2-mEq/kg IV bolus, followed by continuous infusion using a mixture of 150 mEq of sodium bicarbonate added to 1 L of D5W. The IV bolus may be repeated as needed in the case of TCA toxicity.
SUGGESTED READINGS:
- Guidance Document: Management Priorities in Salicylate Toxicity. American College of Medical Toxicology. http://www.acmt.net/cgi/page.cgi/zine_service.html?aid=4210&zine=show.
- Pentel P. Optimal use of bicarbonate therapy. Int J Med Toxicol. 1999;2:3.
- Proudfoot AT, Krenzelok EP, Vale JA. Position paper on urine alkalinization. J Toxicol Clin Toxicol. 2004;42:1. https://pubmed.ncbi.nlm.nih.gov/15083932/
- Woolf AD, Erdman AR, Nelson LS, et al. Tricyclic antidepressant poisoning: An evidence-based consensus guideline for out-of-hospital management. Clin Toxicol. 2007;45:203–233. https://pubmed.ncbi.nlm.nih.gov/17453872/