
This post is an answer to the Case – Epigastric Pain, Vomiting and Elevated Lipase Level
A computed tomographic image showed peripancreatic inflammation and a large fluid collection in the right side of the abdomen that was thought to represent a pancreatic pseudocyst (Panel A, arrow). The patient was treated supportively for acute alcoholic pancreatitis, and percutaneous drainage of the pseudocyst was performed.
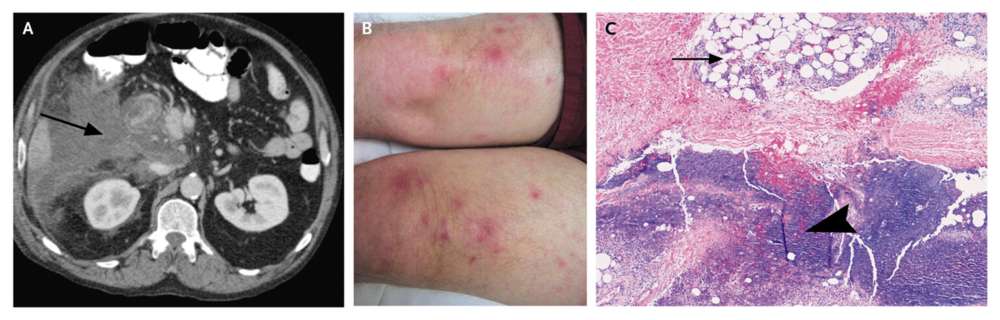
On hospital day five, annular, pink, blanching areas, measuring 2 cm by 2 cm, developed on the distal anterior thighs, with underlying subcutaneous, nontender nodules measuring 1 cm by 1 cm (Panel B), which became increasingly tender during the next several days.
Histopathological examination of a skin-biopsy specimen showed lobular panniculitis (Panel C, arrow), with fat necrosis and focal saponification (arrowhead).
The patient had a prolonged hospital stay and needed total parenteral nutrition and surgery for recurrent pseudocyst. The nodules resolved over the course of 2 weeks.
Pancreatic panniculitis is an uncommon complication of pancreatitis. The liberation of pancreatic enzymes into the circulation causes fat necrosis in distal panni and the formation of subcutaneous nodules. The nodules regress with improvement in pancreatitis.
READ MORE: Acute Pancreatitis: Approach, Evaluation and Management