This post is an answer to the Case – 22-year-old Man With Severe Sudden Onset of Chest Pain
Findings
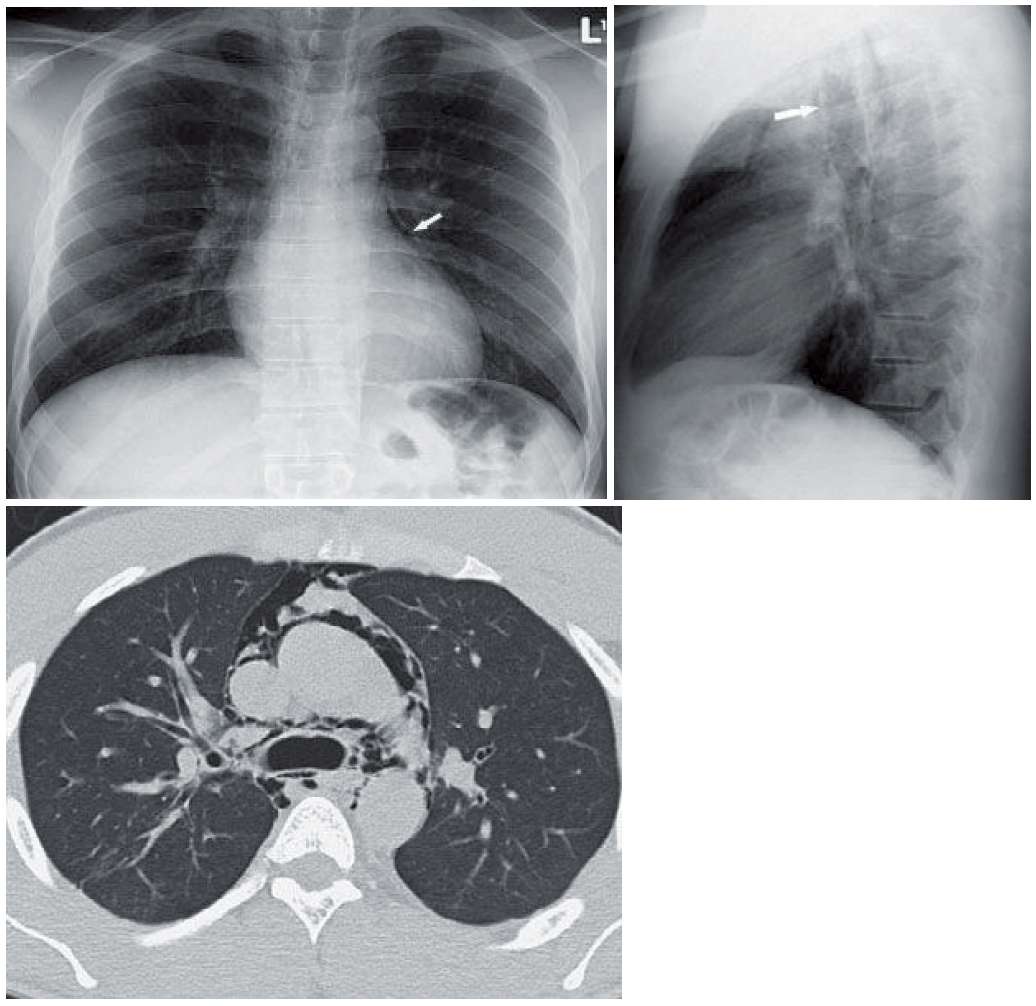
- Chest radiograph shows lucency adjacent to the left heart border (arrow) on the frontal radiograph. Increased lucency is also seen around the aortic arch and in the right paratracheal region.
- On the lateral radiograph, the anterior wall of the trachea is very well seen (arrow on lateral radiograph). Gas is also seen anterior to the ascending aorta.
- CT confirms the presence of gas centrally without fluid or evidence of tracheal rupture.
Differential Diagnosis
Gas adjacent to the left heart border may be from pneumomediastinum, left pneumothorax, or pneumopericardium.
Teaching Points
- The internal webs (multiple radiopaque lines) are more typical of pneumomediastinum.
- Extension above the aortic arch, right paratracheal lucency, and subcutaneous gas are all seen with pneumomediastinum and not pneumopericardium.
- Pneumomediastinum may follow increased thoracic pressure from Valsalva or barotrauma.
- One may see pulmonary interstitial emphysema (PIE) or gas around the pulmonary vessels and bronchi when the etiology is barotrauma.
- Pneumomediastinum may also follow perforation of a hollow viscus (trachea, pharynx, or esophagus). Occasionally, pneumomediastinum may follow pneumoretroperitoneum or perforated bowel.
- Named signs of pneumomediastinum include a continuous diaphragm sign (when the entire diaphragm is seen on the frontal projection); the ring around the artery sign (gas around the extrapericardial pulmonary artery on a lateral projection); and the V of Naclerio (when the gas around the descending artery intersects the gas above the left hemidiaphragm behind the heart).
- Gas between the fascicles of the pectoralis major, also known as the gingko leaf sign, can occasionally be seen.
- Pneumomediastinum will not change appearance with decubitus images; however, pneumopericardium and pneumothorax will rise to the nondependent side.
- Pneumomediastinum may result in a pneumothorax, but pneumothorax should not result in a pneumomediastinum.
Management
- Because pneumomediastinum may be a finding of a ruptured viscus, management is often based on excluding tracheal, pharyngeal, or esophageal rupture. Endoscopy or a fluoroscopic esophageal study may be performed.
- Usually, spontaneous pneumomediastinum resolves in a few days without any intervention.
Further Reading
Bejvan SM, Godwin JD. Pneumomediastinum: old signs and new signs. AJR Am J Roentgenol. 1996 May;166(5):1041-8. doi: 10.2214/ajr.166.5.8615238. PMID: 8615238.