ECG Interpretation
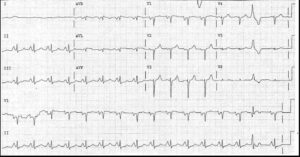
- Sinus rhythm, rate 73/min
- Normal PR interval
- Left Axis Deviation (Left Anterior Fascicular Block (LAFB))
- Normal QRS complexes
- T wave inversion in leads I and aVL
Clinical Intepretation
The left axis deviation indicates a conduction defect in the anterior fascicle of the left bundle branch – Left Anterior Fascicular Block (LAFB). This is due to fibrosis, almost certainly the result of long-standing hypertension.
The T wave inversion in the lateral leads (I and aVL) probably indicates left ventricular hypertrophy (strain pattern), although the QRS complex in lead V6 is not unusually tall and the ‘voltage criteria’ for left ventricular hypertrophy are not met.
What to do?
This man clearly has ‘target organ’ (heart) damage as the result of his hypertension. An echocardiogram should be recorded to assess his left ventricular thickness and function, because the prognosis is worse if there is left ventricular hypertrophy or if there is any reduction in function.
The presence of other risk factors, such as diabetes and hypercholesterolaemia, must be checked and, if necessary, treated. If there is any suggestion of angina, an exercise test should be performed, but if he really is completely asymptomatic this is probably not essential.
Careful control of his blood pressure is the key to management, and since there is evidence of cardiac damage, an angiotensin-converting enzyme inhibitor should be the basis of treatment.
READ ALSO: Summary of ECG Intepretation