ECG Interpretation
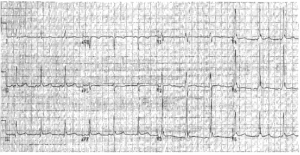
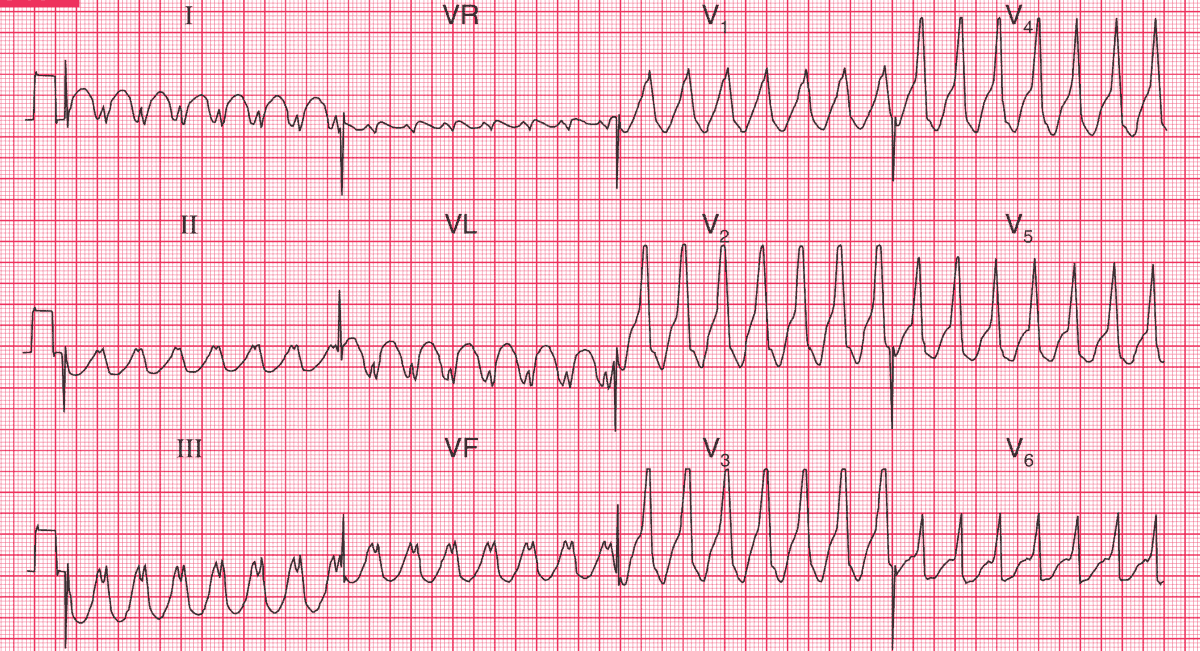
- Broad complex regular tachycardia at 165/min
- No P waves visible
- QRS complex duration about 200 ms
- Concordance of QRS complexes (i.e. all point upwards) in the chest leads
Clinical Interpretation
A broad complex tachycardia can be ventricular in origin, or can be due to a supraventricular tachycardia with aberrant conduction (i.e. bundle branch block). Here the very broad complexes and the QRS complex concordance suggest a ventricular tachycardia.
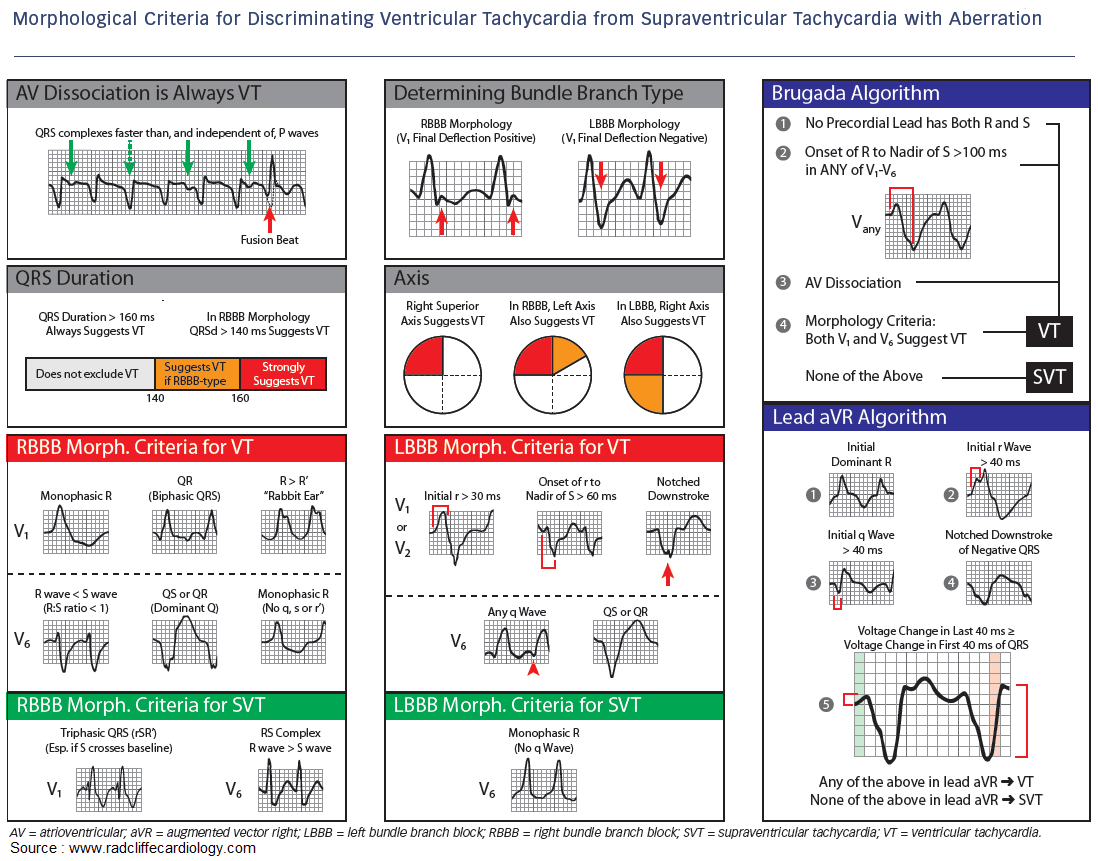
In a patient with a myocardial infarction it is always safe to assume that such a rhythm is ventricular. From the story, one would guess that this patient had a myocardial infarction and then developed ventricular tachycardia, but it is possible that the chest pain was due to the arrhythmia.
What to do ?
This patient has haemodynamic compromise – low blood pressure and heart failure – and needs immediate cardioversion. While preparations are being made it would be reasonable to try intravenous lidocaine or amiodarone.
- READ MORE about:
- MORE Similar Cases: