ECG Interpretation
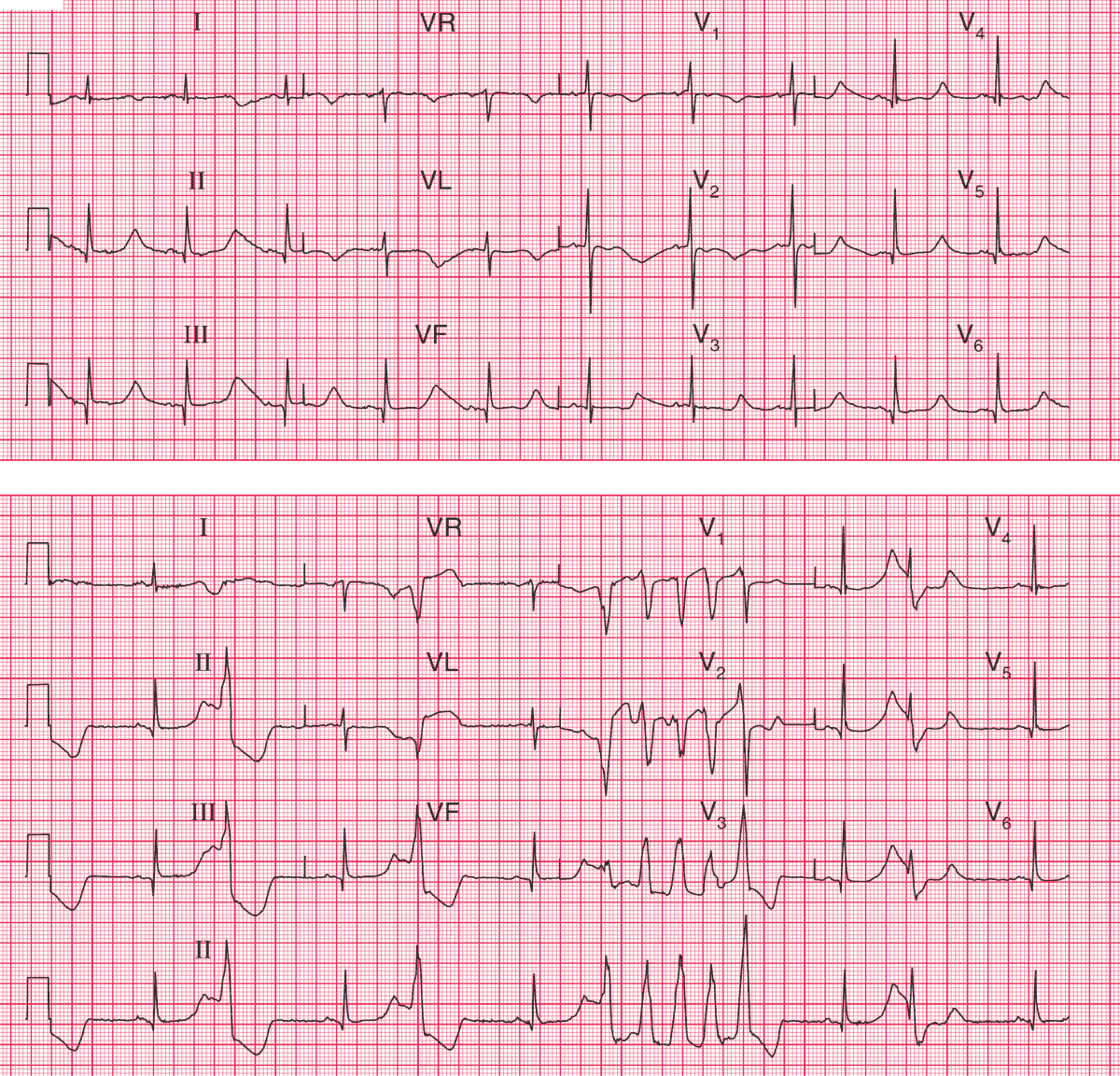
The upper ECG shows:
- Sinus rhythm, with a rate of 60/min
- Narrow Q waves in leads II, III, VF, V4–V6
- Abnormally shaped T waves in most leads
- Prolonged QT interval (about 650 ms)
The lower ECG shows:
- Sinus rhythm with multifocal ventricular extrasystoles
- A run of polymorphic (i.e. changing shape) ventricular tachycardia
Clinical Interpretation
In the upper trace the inferolateral Q waves could represent an old infarction, but they are narrow and are probably septal in origin.
The prolonged QT interval and abnormal T waves suggest either an electrolyte abnormality or that the patient is being treated with one of the many drugs that have these effects. A collapse in a patient with an ECG with a long QT interval suggests episodes of torsade de pointes ventricular tachycardia.
What to do ?
The electrolyte levels, including magnesium, must be checked, and in this case were found to be normal. It is essential immediately to establish what medication the patient is taking, and pending that information it would be sensible to leave her untreated and simply to monitor her for arrhythmias.
It turned out that this woman was taking sotalol – a beta-blocker with class III antiarrhythmic activity which is known to cause QT interval prolongation. When this drug was stopped, her ECG returned to normal.
- READ MORE:
- Similar Cases: