This article is an answer and interpretation of the ECG Case 153
The ECG shows the rhythm is slightly irregular with a rate of 140 bpm. There are no definitive P waves seen before or after any QRS complex, although there are waveforms that may represent atrial activity (+), particularly in leads V4–V6.
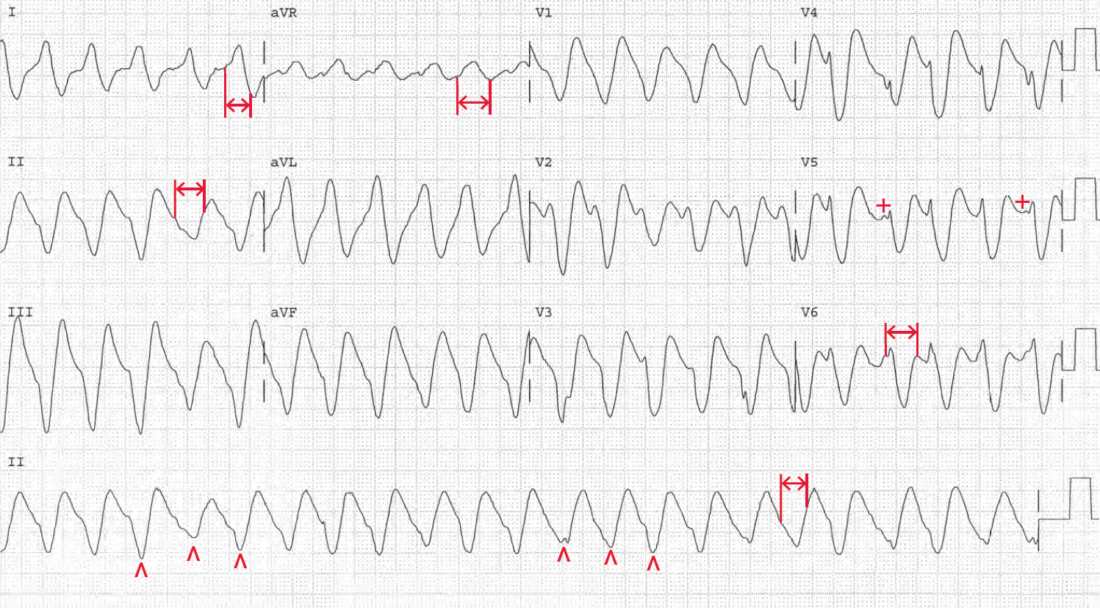
The QRS complex morphology is variable (^) and the duration is prolonged (↔) and also variable (0.28–0.32 sec). The variability in QRS morphology is characteristic of ventricular tachycardia. The markedly prolonged QRS complex duration is seen with hyperkalemia; no other condition, including ventricular tachycardia, prolongs the QRS duration to this extent (ie, ≥ 0.24 sec).
Hyperkalemia often occurs in the presence of hemodynamically significant ventricular tachycardia. This is the result of reduced tissue perfusion, hypoxemia, and acidosis.
The ventricular tachycardia cannot be reverted until the metabolic abnormalities are corrected. Hence hyperkalemia and acidosis should be treated before attempting to revert the ventricular tachycardia, particularly electrical reversion or cardioversion. Cardioversion in the presence of hyperkalemia has a high potential to result in asystole.