This blog post is an answer to the ECG Case 169
There is a regularly irregular rhythm with an average rate of 78 bpm. There appears to be group beating with long (└┘) and short (┌┐) RR intervals. After each long RR interval, there is a QRS complex that ispreceded by a P wave (+) with a PR interval that is short, but constant(0.10 sec). The P wave is positive in leads I, II, aVF, and V4–V6. Hence this is a sinus rhythm with a short PR interval.
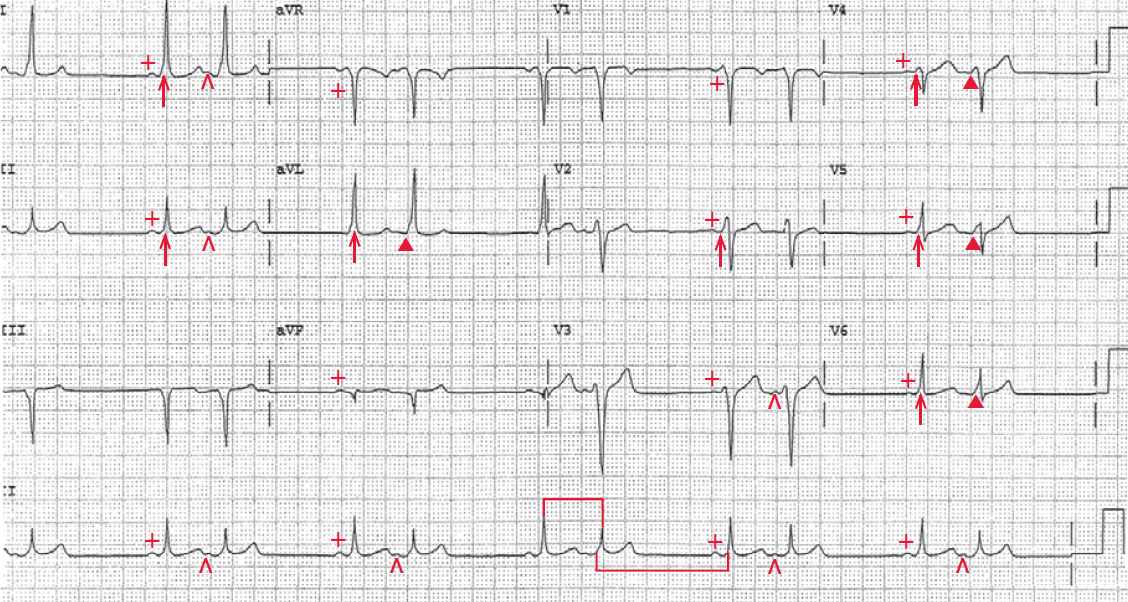
The QRS complex duration is prolonged (0.12 sec), and there is a slurred upstroke to the QRS complex (↑) that is a delta wave. The delta wave causes the base of the QRS complex to be widened, while the rest of the QRS complex is narrow. Hence this is a sinus complex with a Wolff-Parkinson-White (WPW) pattern.
Following this sinus complex, there is an early or premature P wave (^) that is different in morphology from the sinus P wave. This is a premature atrial complex (PAC). As every other complex is an atrial premature complex, this is termed atrial bigeminy.
The PR interval of each of these premature complexes is short and the same as the sinus complexes (0.10 sec) and the QRS complex has a delta wave (▲). However, the QRS complex duration is slightly longer than the sinus complex (0.14 sec) and the delta wave is more prominent, most obviously in leads V4–V6.
The WPW complex represents fusion between conduction via the normal AV node–His-Purkinje system and the accessory pathway.The PR interval and delta wave (and hence QRS complex width) is related to a balance of conduction between these two pathways.
The wider QRS complex and more prominent delta wave indicates that more of ventricular activation of the premature atrial complex is originating via the accessory pathway compared to the sinus complex. This is based on the fact that the premature atrial stimulus occurs at a shortened PP interval and reaches the AV node earlier, before it has completely repolarized. Hence AV conduction velocity is decreased; this is termed decremental conduction, ie, at faster rates, the rate of conduction through the AV node decreases.
While the conduction through the AV node is slower, there is no change in the conduction velocity via the accessory pathway. Hence more of the ventricle is activated via the accessory pathway rather than the normal His-Purkinje system, resulting in a broader delta wave and wider QRS complex.
As initial ventricular activation is through the accessory pathway and the conduction velocity through this pathway is constant, the PR intervals of the sinus complex and premature atrial complex are the same. Another possible cause for the wider QRS complex of the premature atrial complex is that the ectopic atrial focus is closer to the accessory pathway.
The ECG demonstrates QRS complexes that have a WPW pattern. The WPW syndrome represents the arrhythmias that are associated with WPW. The WPW pattern is identified by the electrocardiographic pattern of a short PR interval and a delta wave.