This post is an answer to the ECG Case 185
In the ECG, it should be noted that the rhythm strip is not simultaneous with the 12-lead ECG recording. The rhythm is irregularly irregular with an average rate of 66 bpm. There are no obvious P waves seen. However, there are rapid and irregular undulations of the baseline (^), most obviously seen in leads II, III, and V1–V3. Hence the rhythm is atrial fibrillation.
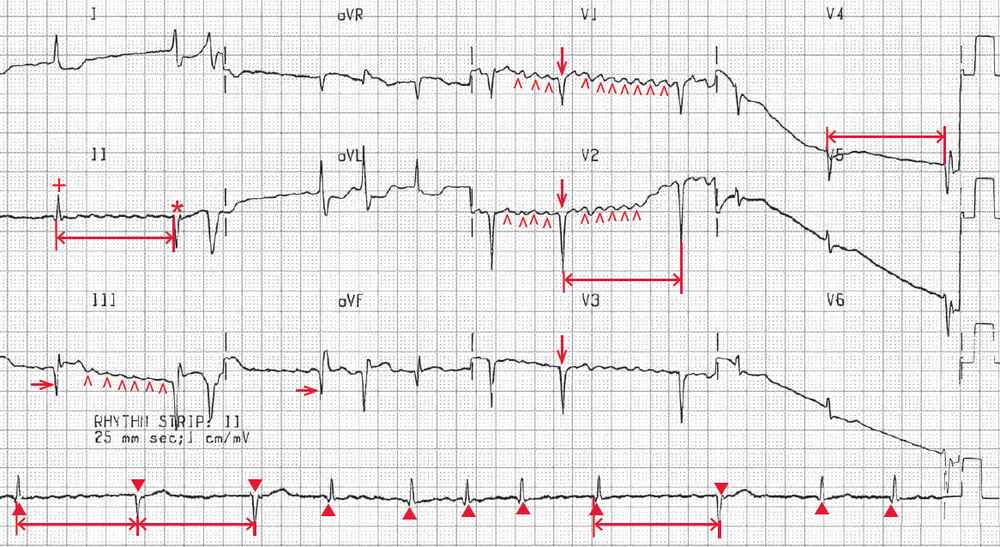
The QRS complex duration is normal (0.08 sec). There are no R waves in leads V1–V3 (↓), consistent with an old anteroseptal myocardial infarction. In addition, there are significant Q waves in leads III and aVF (→), suggesting an old inferior wall myocardial infarction.
Although the QRS complex morphology is consistent, there are changes in the QRS complex axis. All the QRS complexes are positive in lead I and negative in lead aVF. However, it can be seen in lead II that the first QRS complex (+) is positive (and hence associated with a leftward axis between 0º and –30º), while the second QRS complex (*) is negative (and hence associated with a more extreme left axis between –30° and –90°). This can also be seen on the lead II rhythm strip; the first, fourth through eighth, tenth, and eleventh complexes (▲) have a leftward axis, while the second, third, and ninth complexes (▼) have a more extreme left axis.
Also noted is that the complexes with a more extreme left axis always follow a long pause (RR interval) with a rate of 60 bpm, and each time this RR interval is the same (↔). Thus every long RR interval has the same duration (1.20 sec). Therefore, this is intermittent regularization during atrial fibrillation and is characteristic of intermittent complete AV block with an escape QRS complex that always has the same escape interval. The QRS complex following the pause has the same duration and morphology as the conducted QRS complex, the only difference being an axis shift. Hence the escape rhythm is junctional.
Junctional complexes commonly have a slightly different amplitude or axis compared to complexes due to conduction through the AV node. This is likely because the impulse originating from an ectopic junctional focus enters the bundle of His at a different location and is conducted through the His-Purkinje tissue through a different tract compared to impulses coming through the AV node.
In this patient, who appears to be dehydrated as a result of poor oral intake and who is being treated with erythromycin (an antibiotic reported to increase the level of digoxin), the ECG is very suggestive of early digoxin toxicity, with the occurrence of intermittent complete heart block, noted as intermittent regularization of the RR intervals.
Further supporting digoxin toxicity are the symptoms of nausea, vomiting, abdominal pain, and lethargy. Although these are symptoms that can occur with many conditions and are nonspecific, they are frequently seen with digoxin toxicity.
READ MORE:
MORE CASES: