This post is an interpretation of the ECG Case 204
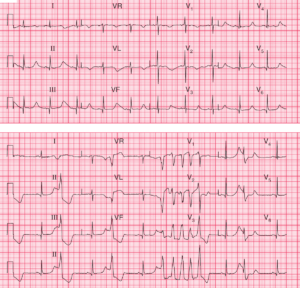
- Rate: ~108 bpm
- Rhythm:
- Sinus rhythm
- Frequent PVCs
- Unifocal
- Single & Couplets
- Evidence of compensatory pauses
- Axis:
- Sinus Complexes – Normal (+70 deg)
- PVC – LAD
- Intervals:
- PR – Normal (~180ms)
- QRS – Sinus Complexes – Normal (100ms)
- QRS – PVCs – Prolonged (120-140ms)
- QT – 320ms (QTc Bazette ~ 420 ms)
- Segments:
- ST Elevation in Leads:
- II (1mm), III (2mm), aVF (3mm)
- ? V6 (0.5mm) – single complex with uneven baseline
- ST Depression in Leads aVL, V1-3
- ST Elevation in Leads:
- Additional:
- T wave inversion in aVR, aVL, V1-3
- P wave inversion in Leads aVR, V1-2
- R wave in V1-3
- PVCs – Discordant T wave & ST segment changes
Interpretation
Acute Inferior and Posterior OMI
What happened next ?
The ECG features were immediately recognized and STEMI protocol was activated. The patient underwent an uneventful transfer for PCI which revealed a 100% occlusion of the proximal RCA which was stented.
The patient was commenced on aspirin, prasugrel, statin, ACE, and beta-blocker therapy. He was discharged after a 3 day in-patient stay.
READ MORE:
SIMILAR CASES: