The ECG shows a regular rhythm at a rate of 100 bpm. There is a P wave (+) before each of the narrow QRS complexes with a stable PR interval (0.16 sec). The P wave is positive in leads I, II, aVF, and V4-V6. Therefore, this is sinus tachycardia.
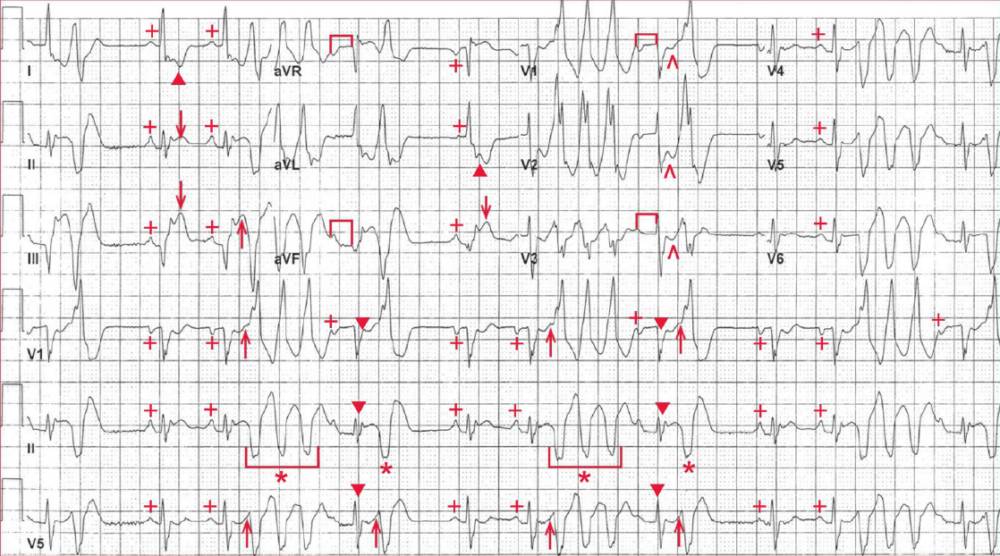
These QRS complexes have a normal duration (0.08 sec) and a left axis, between 0° and -30°, with a positive QRS complex in leads I and II and a negative QRS complex in lead aVF. The QT/QTc intervals are normal (290/440 msec).
There is ST-segment elevation (↓) noted in leads II, III, and aVF, indicating an acute inferior wall myocardial infarction. There is ST-segment depression (▲) in leads I and aVL (which are reciprocal changes) and also in leads V1-V3 (^), which may be reciprocal changes or represent posterior wall involvement.
Also seen are wide QRS complexes (*) (0.16 sec) that are premature and are not preceded by a P wave. They have an abnormal morphology and do not resemble a typical right or left bundle branch block. These are ventricular in origin, and there are single premature ventricular complexes (PVCs) as well as triplets (U) (also termed nonsustained ventricular tachycardia [NSVT]).
Each of the PVCs has the same morphology, and hence they are unifocal. Additionally, each QRS complex of the triplet has the same morphology; hence this is monomorphic NSVT.
After each triplet, there is a sinus complex (▼), but the PR interval is longer (п) (0.26 sec) than the baseline PR interval (0.16 sec). This is a result of retrograde concealed conduction; that is, the ventricular complex preceding this sinus complex results in partial retrograde conduction into the AV node.
However, the impulse does not conduct completely through the node (ie, it is concealed within the AV node), resulting in partial AV nodal depolarization and partial prolongation in its refractoriness. Hence the next atrial waveform gets through the AV node but with a longer conduction time.
Of importance is the fact that the PVCs are very early and are indeed occurring just after the peak of the T wave (↑). These are termed R-on-T PVCs.
This part of the T wave corresponds to the vulnerable period of the fast action potential and is the time immediately after the end of phase 3 and the beginning of phase 4 when the membrane potential transiently becomes more negative (hyperpolarized) than the resting membrane potential of -90 mV.
It is at this time during the action potential when an electrical stimulus of enough energy can provoke ventricular flutter, polymorphic ventricular tachycardia, or ventricular fibrillation.
- READ MORE:
- Know the Differential for ST Segment Elevation: It’s More Than Just ACS
- Remember to Obtain a Rightsided ECG in a Patient with an Inferior Myocardial Infarction
- Know the Mimics of Ventricular Tachycardia
- Never Mistake Ventricular Tachycardia for Supraventricular Tachycardia with Aberrant Conduction
- ECG Interpretation: All you need to know