This post is an answer to the ECG Case 211
- Rate: ~84 bpm
- Rhythm: Regular
- Axis:
- Normal (~75 deg)
- Intervals:
- PR – Normal (200ms)
- QRS – Normal (100ms)
- QT – 360ms (QTc Bazette ~ 425 ms)
- Segments:
- ST Elevation in lead aVR ~0.5mm
- ST Depression
- Horizontal in leads V2-V4
- Concave in leads II, aVF, V5-V6
- Additional:
- T wave inversion in lead V1
- Flat T waves in II, III, aVF, aVL, V5, V6
- Notching terminal portion QRS complex in leads II, V5, V6
- R/S Ratio V2=0.85
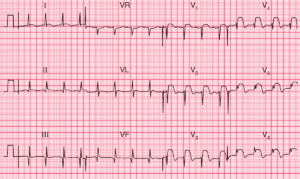
Interpretation
Highly suspicious ECG for Posterior MI.
- Flat right precordial ST depression
- Prominent R wave V2, although R/S <1
- Infero-lateral ST depression
What happened next ?
Well the patient had posterior leads performed, ECG below. You can see leads V1 and V3 have been moved to the posterior region and re-labelled as V7 & V9. This configuration is due to our local lead set up which uses only two physical leads with multiple connectors on each to record the twelve lead.
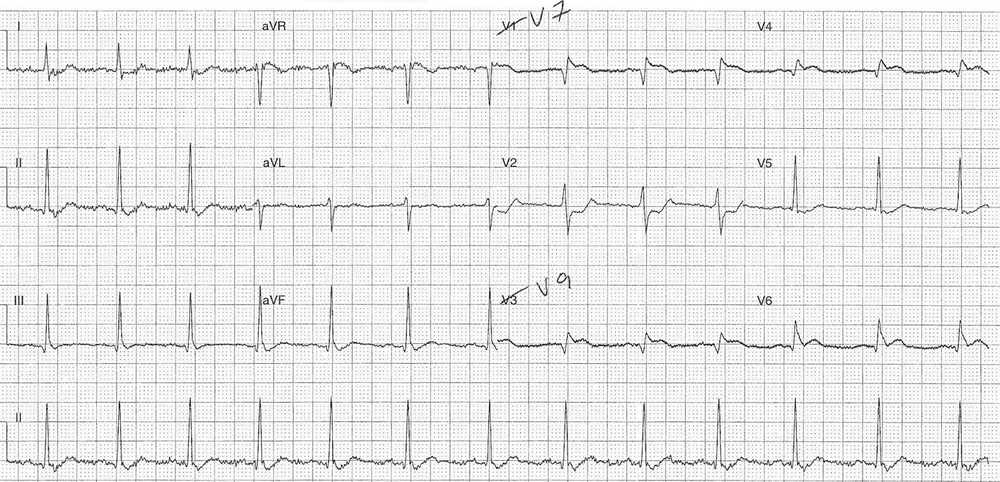
As you can see there is ST elevation in lead V7 (1mm) and V9 (~0.5mm) which is diagnostic of an isolated posterior infarction.
The patient was transferred for urgent coronary angiography and PCI.
His angiography showed:
- Left main – irregularities
- Left anterior descending – 40-50% mid vessel stenosis
- Left circumflex – proximal occlusion
- Right coronary – proximal occlusion with bridging collaterals
- Ventriculogram – normal
His proximal circumflex lesion was stented acutely, and he was discharged following a 4 day in-patient stay.
SIMILAR CASES: