This post is an answer to the ECG Case 299
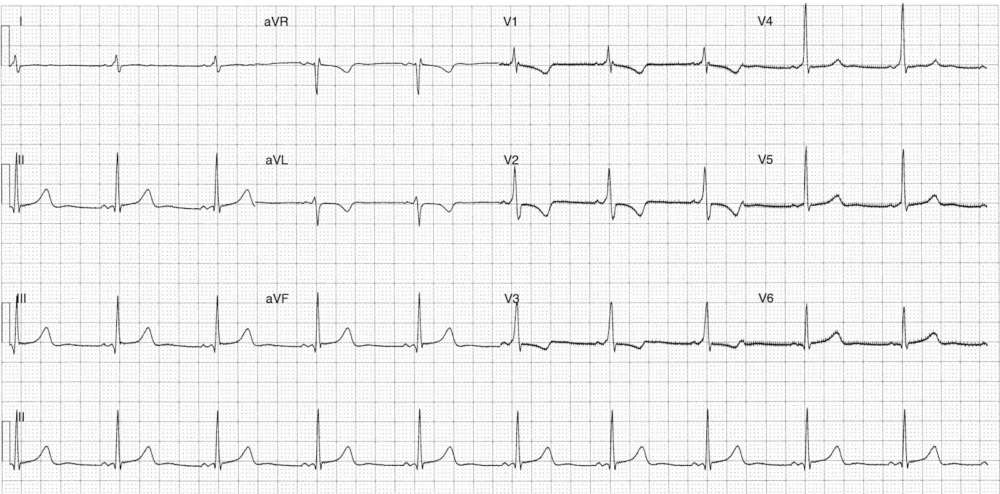
- Rate: 60
- Rhythm: Sinus arrhythmia
- Axis: Normal
- Intervals:
- PR – Short (~100ms)
- QRS – Prolonged (120-130ms)
- QT – 440ms (QTc Bazette 440 ms)
- Segments:
- ST elevation in leads III, aVF <1mm with flat morphology
- Additional:
- Delta waves in leads I, V1-4
- Pseudo right ventricular hypertrophy secondary to pre-excitation rather than actual chamber enlargement with the following ECG features:
- Dominant R wave in leads V1-6
- R/S ratio > 1 in lead V1
- T wave inversion in leads aVL, V1-3
Interpretation
- Wolff-Parkinson-White Syndrome
- Left posterior / left posterolateral accessory pathway using Arruda algorithm
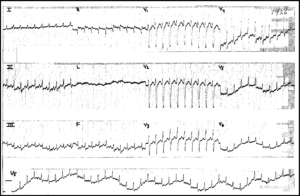
What happened next ?
The patient had known pre-excitation and had been non-compliant with beta-blocker and sodium-channel blocker therapy. The patient was admitted for telemetry and re-instigation of anti-arrhythmic agents prior to ablation consideration / planning.
SIMILAR CASES: