This post is an answer to the ECG Case 328
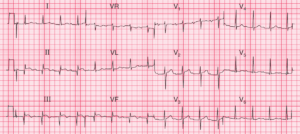
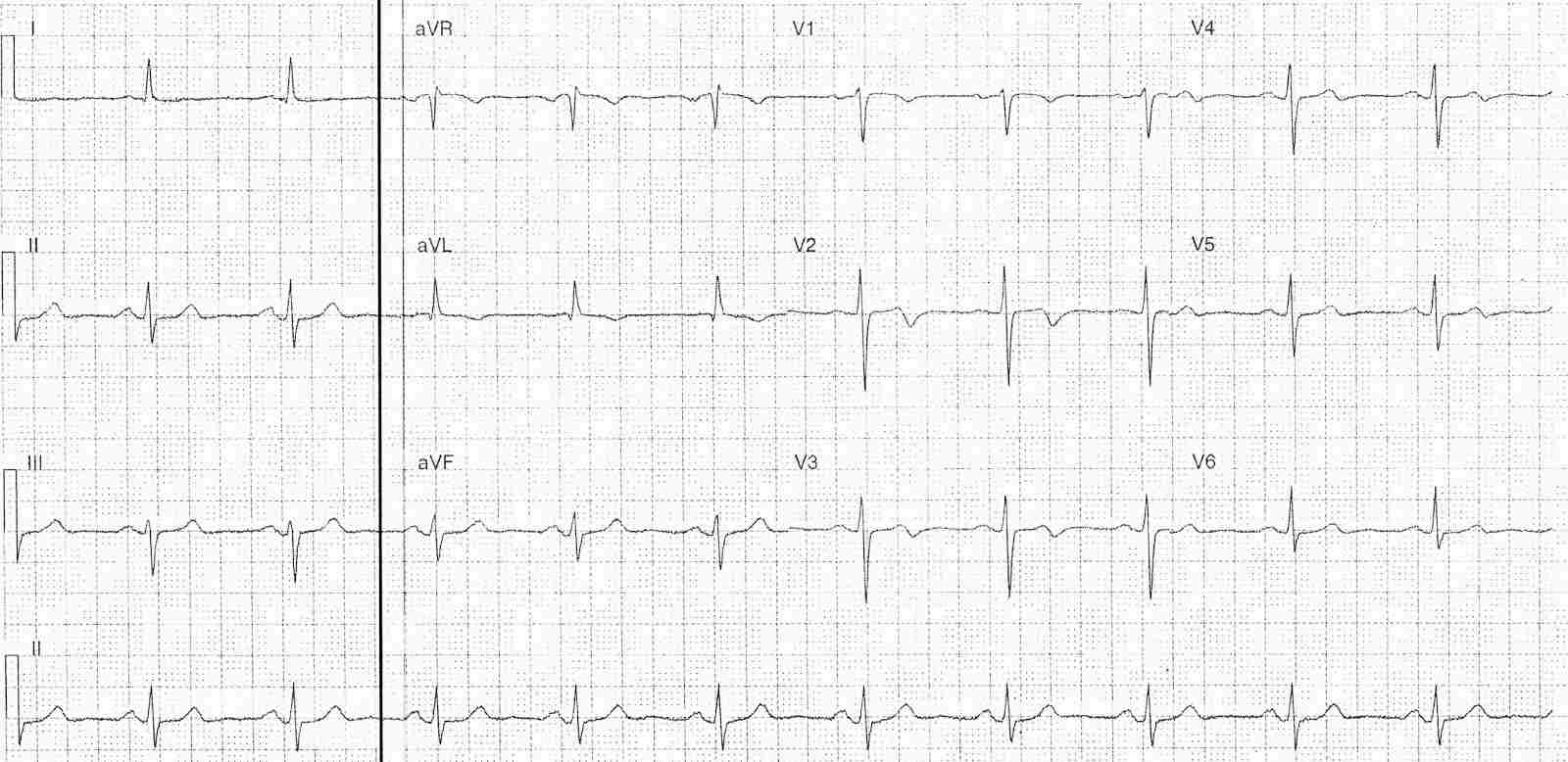
Pain free ECG
- Regular sinus rhythm rate ~60-65 bpm
- Normal axis
- Biphasic T wave in leads V2-4
- Positive to negative deflection
- T wave inversion in lead aVL
- Flat T wave in lead I
- Subtle ST elevation in aVR and V1
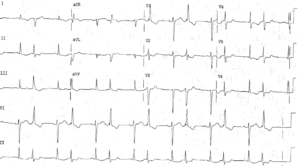
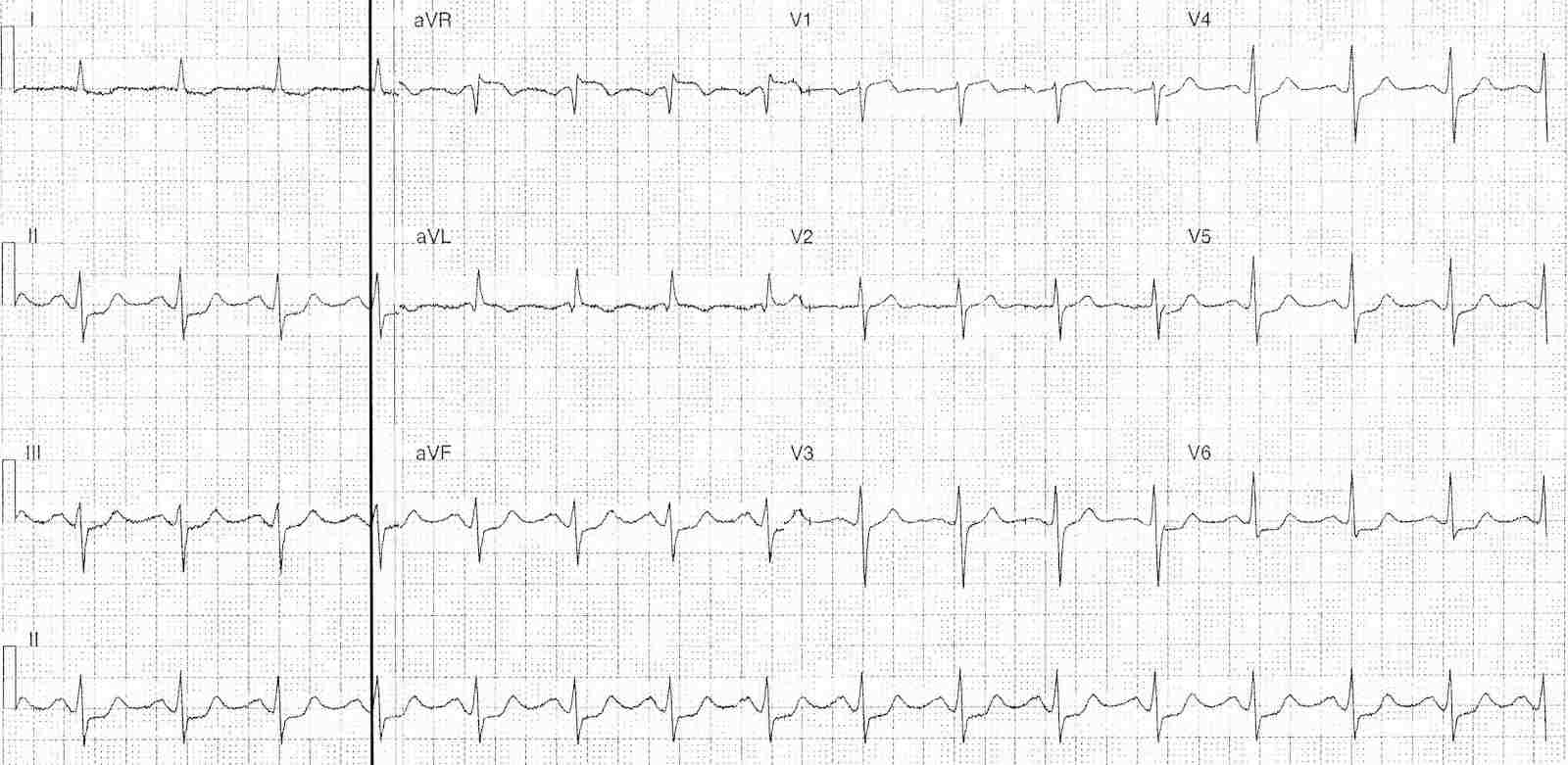
ECG with chest pain
- Regular sinus rhythm rate 96 bpm
- ST Elevation in leads aVR (1mm) , V1 (1mm) and aVL
- ST Depression in leads I, II, III, aVF, V3-6
- Note T inversion on pain-free ECG now positive deflection only
Interpretation
- Serial ECGs showing dynamic ST and T wave changes
- Pain-free ECG’s showing Wellen’s pattern
- During episode of chest pain
- Pseudo-normalisation of T wave changes
- Associated diffuse ST depression and ST elevation in aVR and V1
What happened next ?
The patient was treated with dual anti-platelet therapy, heparinised and admitted under cardiology. She had a troponin (cTnI) of 0.22 ug/L and remained pain-free. Her angiogram showed:
- LMCA: Irregularities
- LAD: Proximal / Mid 70-80% culprit stenosis -> Stented
- Cx: Irregularities
- RCA: Irregularities
Subsequent echo was essentially normal without wall motion abnormality or decreased ejection fraction.
![Read more about the article Atrial Flutter: ECG Interpretation [With Examples]](https://manualofmedicine.com/wp-content/uploads/2022/01/Atrial-Flutter-with-4-1-AV-Block-300x135.png)