This post is an answer to the ECG Case 335
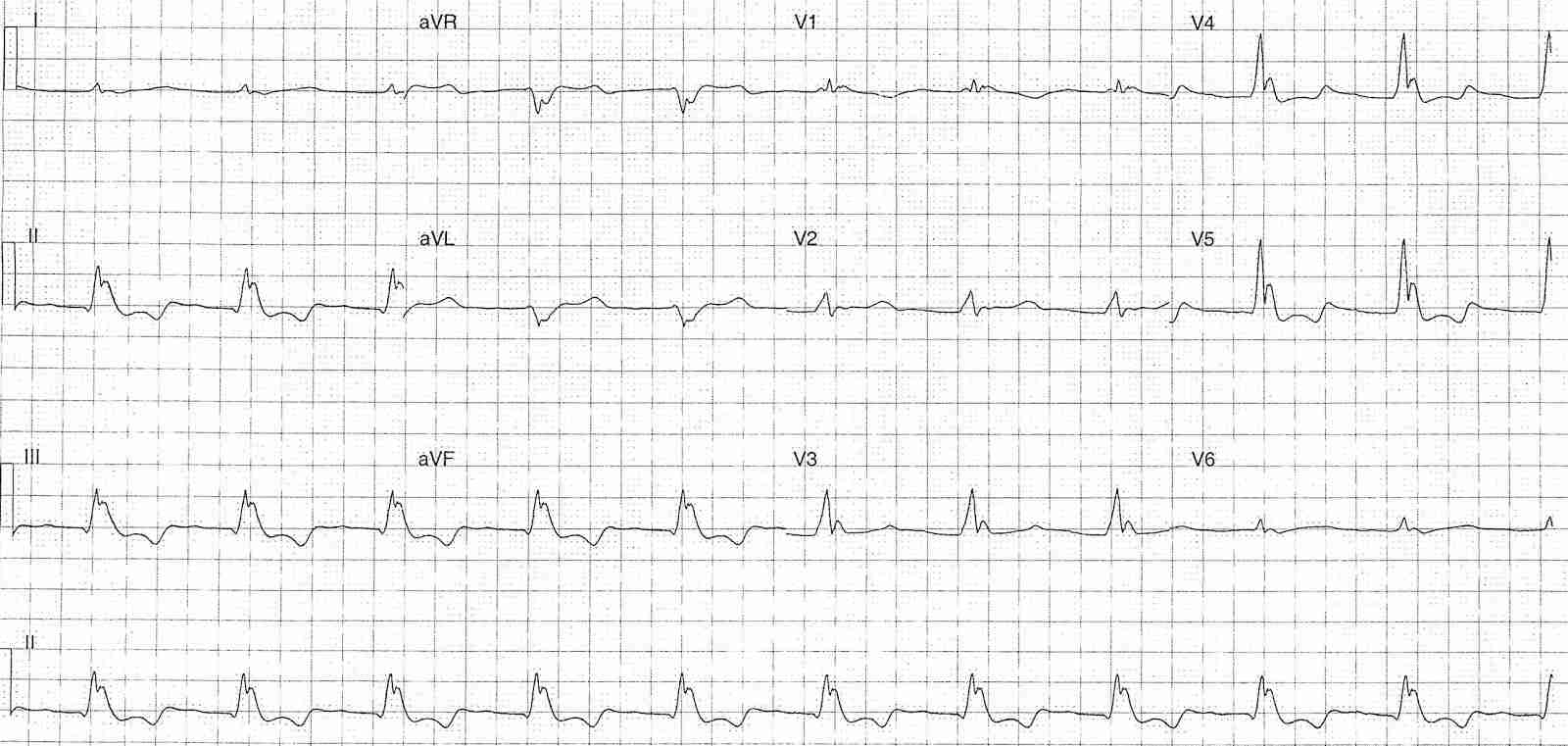
- Rate: 66 bpm
- Rhythm:
- Regular
- No clear p waves
- Axis: Normal
- Intervals:
- QRS – Prolonged (240ms)
- QT – 520ms (QTc Bazette 545 ms)
- Additional:
- J waves in leads II, III, aVF, V2-6
- ST Depression in leads II, III, aVF, V4-5
- Subtle ST elevation in leads aVR and aVL
- T wave inversion in leads II, III, aVF
- Biphasic T wave in leads V4-5 possible T-U fusion
Several differentials for these ECG features especially given clinical scenario include:
- Hypothermia – must likely – junctional / escape rhythm, J waves, QT & QRS prolongation
- Intracerebral pathology – can cause J waves and QT prolongation
- Drug toxicity – loss of normal sinus rhythm, can cause J waves, QRS and QT prolongation, also can be a cause of hypothermia
Remember J waves are not pathognomonic of hypothermia and can be seen in association with hypercalcaemia and raised ICP.
What happened ?
The patient had multiple acute medical issues:
- Severe hypothermia – core temperature 25.9 C (78.6 F)
- Coma – GCS 3 (E=1, M=1, V=1)
- Hyperkalaemia (7.2 mmo/L) and acute renal failure
- Hepatic failure with coagulopathy
- Likely polypharmacy overdose
Despite early aggressive resuscitation, rewarming and renal replacement therapy the patient had progressive multi-organ failure and did not survive.
READ ALSO: Hypothermia Algorithm
SIMILAR CASES: