This post is an answer to the Case – Loss of Conscious after Severe Headache
CT Interpretation
Hyperdense blood in the anterior interhemispheric fissure, bilateral Sylvian fissures, basal cisterns, ventricles and cortical sulci and the intraventricular extension of haemorrhage into the lateral and 4th ventricles.
In simplistic terms, the normal CSF spaces are ‘black’, but in this case all the CSF spaces are ‘white’ because of the presence of fresh blood.
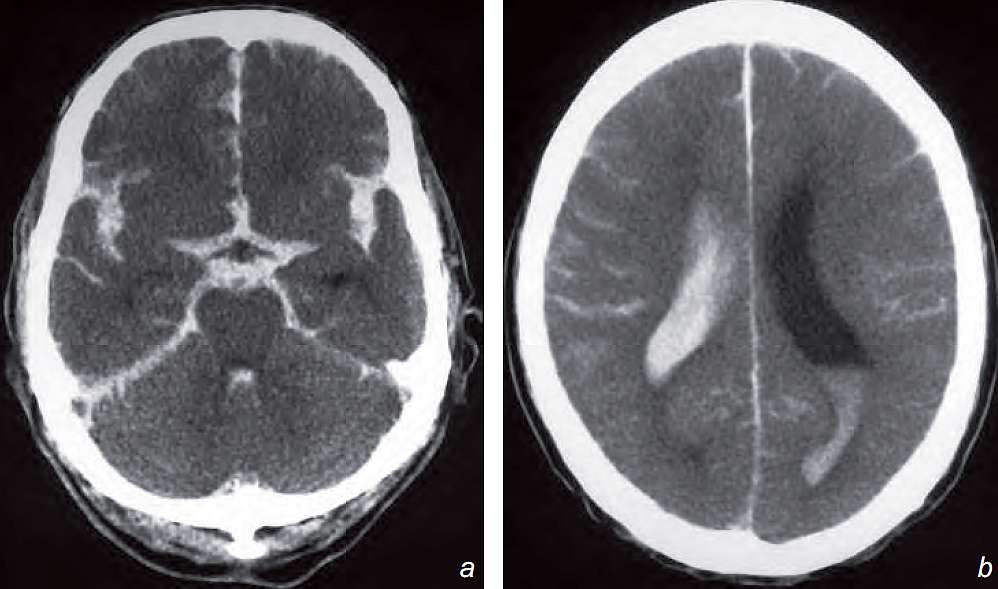
Diagnosis: Acute Subarachnoid Haemorrhage
The most likely cause of SAH is a ruptured aneurysm and further investigations such as a CT angiogram (CTA)/digital subtraction angiogram (DSA) may be required to identify the source of the bleeding.
Discussion
Underlying etiology:
- Aneurysm, 90% of the cases
- Arterio-venous malformation (AVM)
- Coagulation disorder
- Extension from intra-parenchymal haemorrhage
- Trauma
- Idiopathic
Complications
- Rebleed 50% rate within the first two weeks
- Hydrocephalus due to ventricular obstruction or arachnoiditis
- Vasospasm, ischaemia, infarction
- Leptomeningeal superfi cial siderosis, cranial nerve (particularly I, II, VIII) palsies
- Neurological pulmonary oedema
Investigations
- CT is the initial imaging investigation of choice:
- Highly sensitive in detecting acute subarachnoid blood within the first 48 hours
- The bleeding source may be close to where there is the largest amount of blood and associated intraparenchymal haemorrhage is demonstrated
- Angiogram
- The aim of CTA/DSA is to confirm the diagnosis, locate the aneurysm, identify any other aneurysms (known association of multiple intracranial berry aneurysms with adult polycystic kidney disease)
READ MORE: Diagnosing the Patient with Loss of Consciousness (Syncope and Coma)
SIMILAR CASE: Patient with Decreased Level of Consciousness