This post is an answer to the Case – A Pigmented Skin Lesion that has Gotten Bigger
What features suggest that this is a malignant melanoma?
The story of recent enlargement is important. Careful inspection shows irregularity in its outline, its surface and its pigmentation – all highly suspicious.
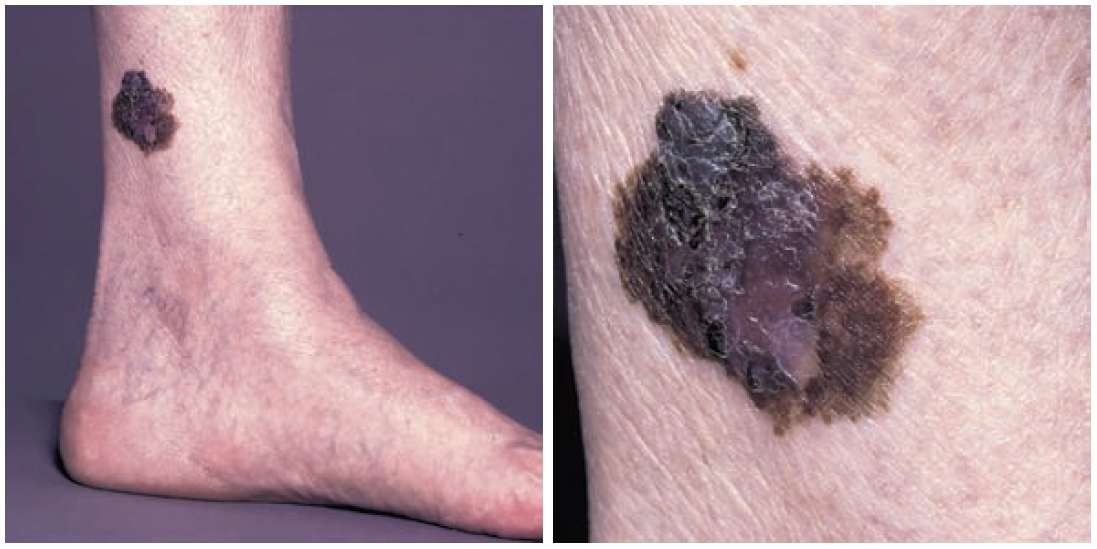
What other features, not present in this patient, indicate malignant change?
Other features are bleeding, ulceration, spread of pigment beyond the edge of the tumour and surrounding daughter nodules. A history of itching or pain is also suspicious.
Where would you examine the patient next for evidence of metastatic spread?
Examine all the way along the lower limb for the presence of satellite nodules deposited along the lymphatics. Carefully examine the groin for inguinal lymphadenopathy.
Where else, apart from the skin, may malignant melanomas occur?
Malignant melanomas may occur on the mucosa of the nose, mouth, anal canal and intestine. In the eye, malignant melanomas may be found in the conjunctiva, choroid and pigmented layer of the retina.
What factors determine the prognosis in patients with cutaneous malignant melanomas?
The prognosis in a case of cutaneous malignant melanoma depends on the following:
- The thickness of the primary tumour (the Breslow depth). If this is less than 0.75 mm, the outlook is excellent. The deeper the lesion, the worse becomes the survival rate; this is associated with the greater danger of lymphatic spread as the invading tumour reaches the lymphatic vessels, which lie in the dermis.
- A superficial spreading lesion has a better prognosis than a penetrating and ulcerating melanoma – for exactly the same reason.
- Melanomas on the limbs have a better prognosis than those of the trunk, the eye and the viscera.
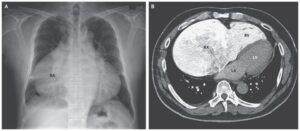
- The presence of cutaneous or lymphatic deposits greatly increases the gravity of the prognosis, while blood-borne metastases, for example to the liver, make the prognosis virtually hopeless.
This patient was treated along standard lines. What are these?
- The lesion was excised and the diagnosis confirmed histologically by frozen section. A wider local excision was then performed with a clearance of 1 cm for every millimetre of Breslow depth of the lesion and the defect repaired by means of a split-skin graft taken from the other thigh
- The sentinel lymph node in the groin was identified by injection of blue dye around the melanoma preoperatively and was excised – in this case it was free of tumour.
- At follow-up a careful check was performed at each visit on the local area, the skin along the line of the lymphatics of the lower limb and the groin lymph nodes.
- Should inguinal node metastases develop, a block dissection of the groin would be performed.
SIMILAR CASES: