
This post is an answer to the Case – Patient with Lethargy, Polydipsia and Polyuria
What abnormalities do you see on the radiographs ?
- Frontal view of hand:
- Generalized osteopenia
- Cortical bone tunneling
- Subperiosteal bone resorption
- Lateral skull view:
- Mottled calvarium (salt and pepper skull)
- Blurred inner and outer tables
- Well-defined lucent lesion in the parietal bone
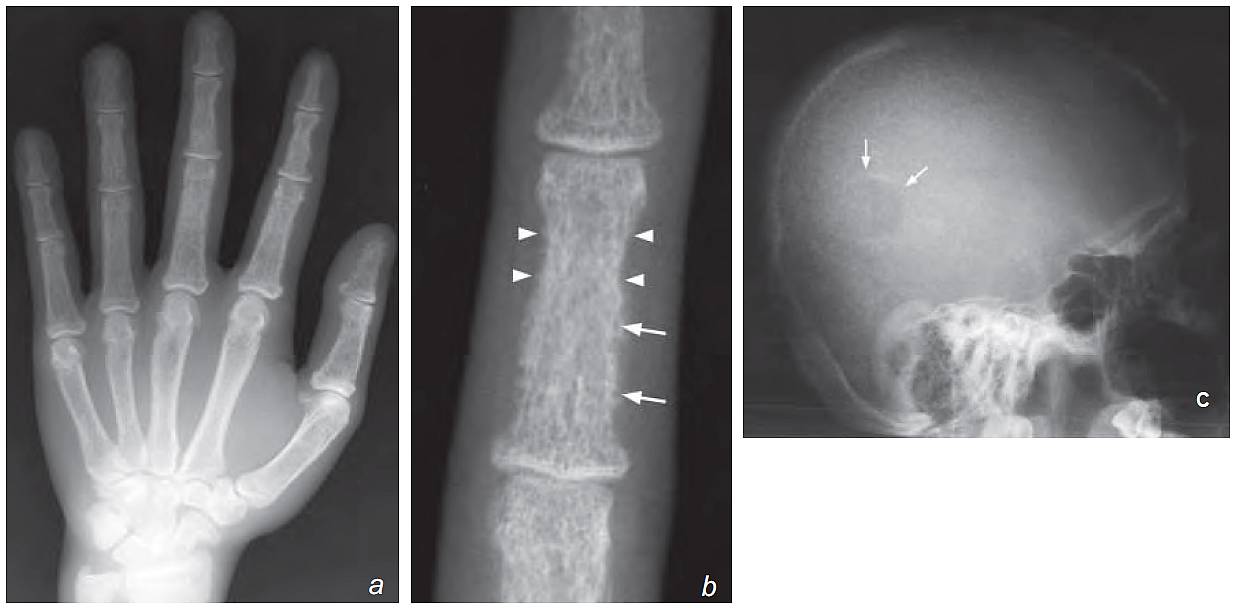
b) Magnifi ed view of the third middle phalanx shows a lace-like cortex due to bone resorption and enlargement of the Haversian canals (latter seen as the numerous holes in the cortex, [arrows]). There is also subperiosteal bone resorption (arrowheads).
c) Lateral view of the skull shows blurring of inner and outer tables of the skull (normally of distinct borders). There is also a generalized mottled appearance which is due to widespread granular bone resorption. This is termed a salt and pepper skull. There is a well-defined lucent lesion in the parietal bone indicating a Brown tumour (arrows)
Diagnosis: Hyperparathyroidism
Discussion
This is a disease due to over-activity of the parathyroid gland. It may be: primary, due to a parathyroid adenoma; secondary, due to chronic renal disease leading to loss of calcium and phosphorus; tertiary, parathyroid glands acting independent of calcium homeostasis after prolonged secondary hyperparathyroidism. Increased parathormone (PTH) results in increased osteoclast activity, leading to increased bone resorption and increased serum calcium levels.
The radiographic findings reflect some of the pathology, including:
- Subperiosteal outer cortical bone resorption – most prominent in middle phalanx of 2nd and 3rd fi ngers
- Cortical tunneling – bony resorption within Haversian canals of cortex.
- Lace-like appearance of bone cortex due to a combination of the above signs
- Apparent joint-space widening due to bone resorption
- Brown tumour (osteoclastoma) – well-defined cystic lesion in affected bone, representing a focal mass of osteoclasts and fibrous tissue . Commonly in skull, femur and pelvis.
- Insufficiency fractures as a result of the weakened bones
- Soft tissue/vascular calcification – due to high serum calcium levels
- Chondrocalcinosis – calcification within cartilages
Bone scan may show a ‘superscan’ where there is diffuse increase in uptake in the entire skeleton due to increased bone activity.
Parathyroid adenoma is the underlying cause in majority (~80-90%) of cases. Other less common causes include parathyroid hyperplasia and parathyroid carcinoma.
Ultrasound of neck is sensitive in detecting parathyroid and helps the surgeon to accurately localize the lesion before surgery. If an ultrasound cannot detect a parathyroid lesion in a patient with biochemical evidence of hyperparathyroidism, radionuclide MIBI scan should be used to detect a hyperfunctioning adenoma.
Role of imaging in patients with hyperparathyroidism
- Demonstrate bone and soft tissue changes radiographically as a baseline for monitoring progress
- Demonstrate complications such as Brown tumours or insufficiency fractures
- Identify/localize a parathyroid adenoma
Summary
- Hyperparathyroidism is a clinical diagnosis, based on biochemical tests.
- Subperiosteal, outer cortical and periarticular bony resorption are characteristic radiograph findings, most commonly demonstrated on plain radiograph of hands.
- Ultrasound neck or radionuclide MIBI scan help pre-operative localization of a parathyroid adenoma.