This article is an answer to the Case – 11-year-old Boy With Retrosternal Chest Pain
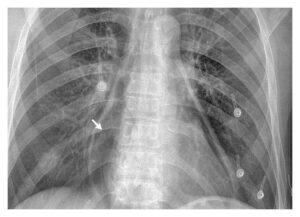
Chest radiograph revealed a large retrosternal mass in the mediastinum with some displacement of the trachea.
CT imaging of the chest, abdomen and pelvis revealed enlarged lymph nodes in the neck and supraclavicular fossa bilaterally. There were multiple nodes in the mediastinum with the largest measuring 5.7 x 5.2 x 9.8 cm (image below). It also demonstrated enlargement of the liver and spleen.

He was subsequently diagnosed with Hodgkin Lymphoma (HL) following a surgical biopsy of a superficial cervical lymph node.
Imaging studies in Hodgkin Lymphoma (HL)
Imaging studies that should be undertaken when Hodgkin Lymphoma is suspected include chest radiography with AP and lateral views to assess the bulk of the mediastinum. CT/MRI of the neck, chest, abdomen and pelvis are also useful to assess the extent of the disease and look for extranodal involvement.
Ultrasound scanning has a small role to play in the initial diagnosis but can be used for follow up and monitoring particularly of cervical nodes, as it is relatively simple and non-invasive.
Fluorodeoxyglucose (FDG) positron emission tomography (PET) has a proved role for HD in adults but the role of this imaging technique is as yet uncertain in children. However, it may play a role in distinguishing between benign masses and active disease post treatment.
No single imaging technique can provide a definitive diagnosis and lymph node biopsy remains the gold standard for diagnosis as fine-needle aspiration is not recommended because of lack of stromal tissue obtained which leads to difficulty classifying the Hodgkin lymphoma.
References
- Dunn, R, Dilley, S et al (2006) The Emergency Medicine Manual. 4th Edition
- Küppers, R (2009) The biology of Hodgkin’s lymphoma. Nature Reviews: Cancer 9:15-27
- Kumar,P, Clark, M (2006) Clinical Medice. 6th Edition
- Thomas RK, Re D, Wolf J, Diehl V (2004) Part I: Hodgkin\’s lymphoma-molecular biology of Hodgkin and Reed-Sternberg cells. Lancet Oncol 5:11-18 (PMID: 14700604)
- Toma P, Granata C, Rossi A, Garaventa A (2007) Multimodality Imaging of Hodgkin Disease and Non-Hodgkin Lymphomas in Children. RadioGraphics 27:1335-54 (PMID: 17848695)
- Hudson MM, Krasin MJ, Kaste SC (2004) PET imaging in pediatric Hodgkin\’s lymphoma. Pediatric Radiology 34:190-198 (PMID: 14745528)
- Juweid M, Vose J (2010) Imaging in Early-Stage Hodgkin\’s Lymphoma. The New England Journal of Medicine 362:962 (PMID: 20220198)