
This article is an answer to the Case – Right Sided Pleuritic Chest Pain
Because of his new symptoms a chest radiograph was done which unexpectedly revealed a large right paracardiac soft tissue density mass. A CT thorax was thus performed to investigate this further.
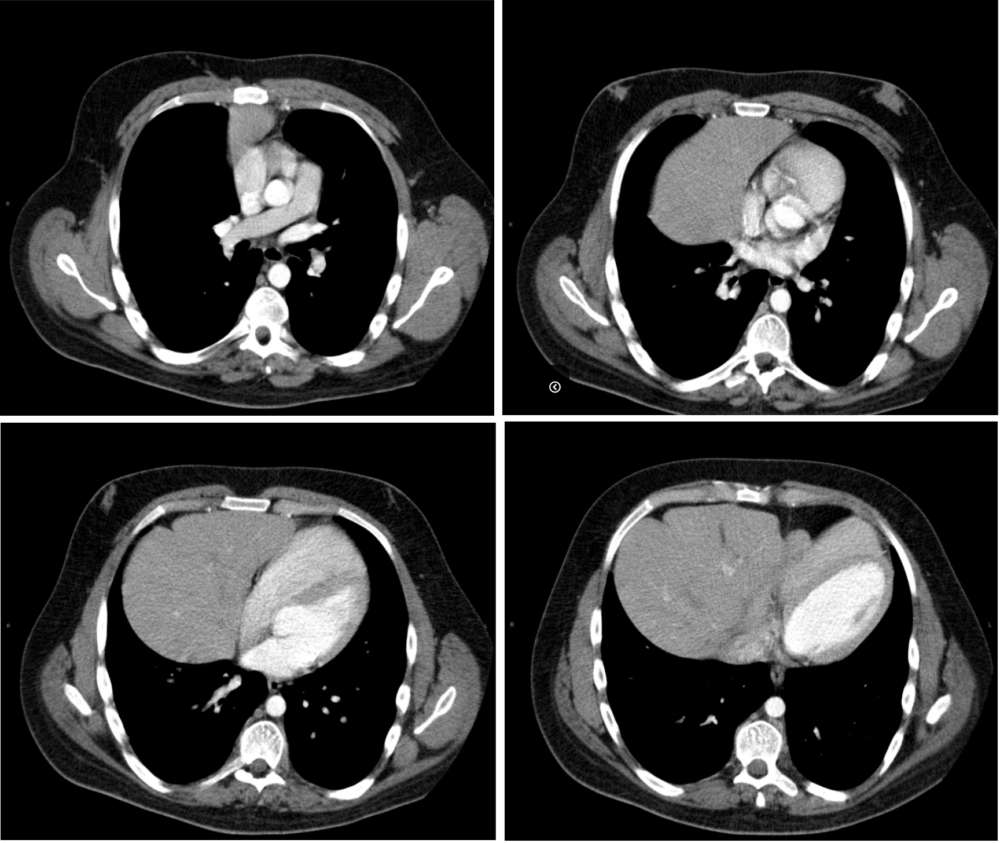
Axial CT images through lower thorax with intravenous contrast demonstrating the herniation of the left lobe of the liver together with the Gallbladder,and part of the stomach and transverse colon into the thorax via a ventral diaphragmatic defect.
Discussion
The two main types of diaphragmatic hernia known are:the Bochdalek’s hernia, involving the posterior portion of the diaphragm which is usually left sided, and Morgagni’s hernia, involving the anterior diaphragm usually located on the right side.
The Morgagni hernia was first described in 1761 and accounts for 3%-4% of all diaphragmatic defects. It is the least common of the congenital diaphragmatic Hernias (CDHs).
The majority of Morgagni hernias are diagnosed in children who usually present symptoms of pneumonia or sepsis. Although adult patients are usually asymptomatic, they may present with dyspnea, chest discomfort or pain, and chronic gastrointestinal symptoms. Less commonly, symptoms resulting from intestinal strangulation or obstruction and gastric volvulus formation have also been reported.
Morgagni hernias may be diagnosed incidentally during either abdominal operation or on routine chest radiography. This may be suspected when a chest radiograph shows a paracardiac mass or a gas-fluid level at the mediastinum corresponding to the herniated bowel or stomach. The Morgagni hernia can be mistaken for lung consolidation or abscess, mediastinal tumour and pleuropericardial cyst.
Congenital diaphragmatic defects in children have a high mortality due to pulmonary hypoplasia and pulmonary hypertension.Herniation of liver is a bad prognostic sign. While most symptomatic adult patients with left-sided diaphragmatic defects present with symptoms of visceral herniation, it is believed that right-sided agenesis occurs with few symptoms due to the presence of the liver preventing other viscera from herniating through the diaphragmatic defect.
Diagnostic imaging modalities to assess diaphragmatic defects range from routine chest radiographs to magnetic resonance imaging. Contrast radiography may be of assistance in determining the presence of intrathoracic bowel herniation. Solid organ herniation may be more difficult to diagnose and may require computed tomography. Further imaging is necessary when symptoms are more subtle or patients are asymptomatic. In these instances, thin slices and multiplanar images can assist in tetsablishing the diagnosis. Ultrasound may be of complementary value by demonstrating the free edge of the diaphragm defect within pleural fluid or demonstrating liver herniation.
References
- Gale ME. Anterior diaphragm: variations in the CT appearance. Radiology. 1986 Dec;161(3):635-9. (PMID: 3786709)
- Kleinman PK, Raptopoulos V. The anterior diaphragmatic attachments: an anatomic and radiologic study with clinical correlates. Radiology. 1985 May;155(2):289-93. (PMID: 3983375)
- Popovic T, Nikolic S, Radovanovic B, Tomislav J. Missed diaphragmatic rupture and progressive hepatothorax, 26 years after blunt trauma. European journal of Trauma, 2004;30:43-6.
- Erdem LO, Erdem CZ, Comert M. Intrapancreatic lipoma and Morgagni hernia: a previously unrecognized association. Dig Dis Sci. 2004 Nov-Dec;49(11-12):1962-5. (PMID: 15628734)
- Komanapalli CB, Velamoor GR, Schipper PH, Sheppard B, Sukumar SM. Peripartum Diagnosis and Management of Diaphragm Agenesis. CTSNet.
- Ng CSH, Lee TW, Wan S, Yim APC. Caval foramen hernia masquerading as a thoracic mass. Canadian Journal of Surgery, 2006;49:64-6.
