
This post is an answer to the Case – Chest Pain and Shortness of Breath After Being Shot in the Back
Findings
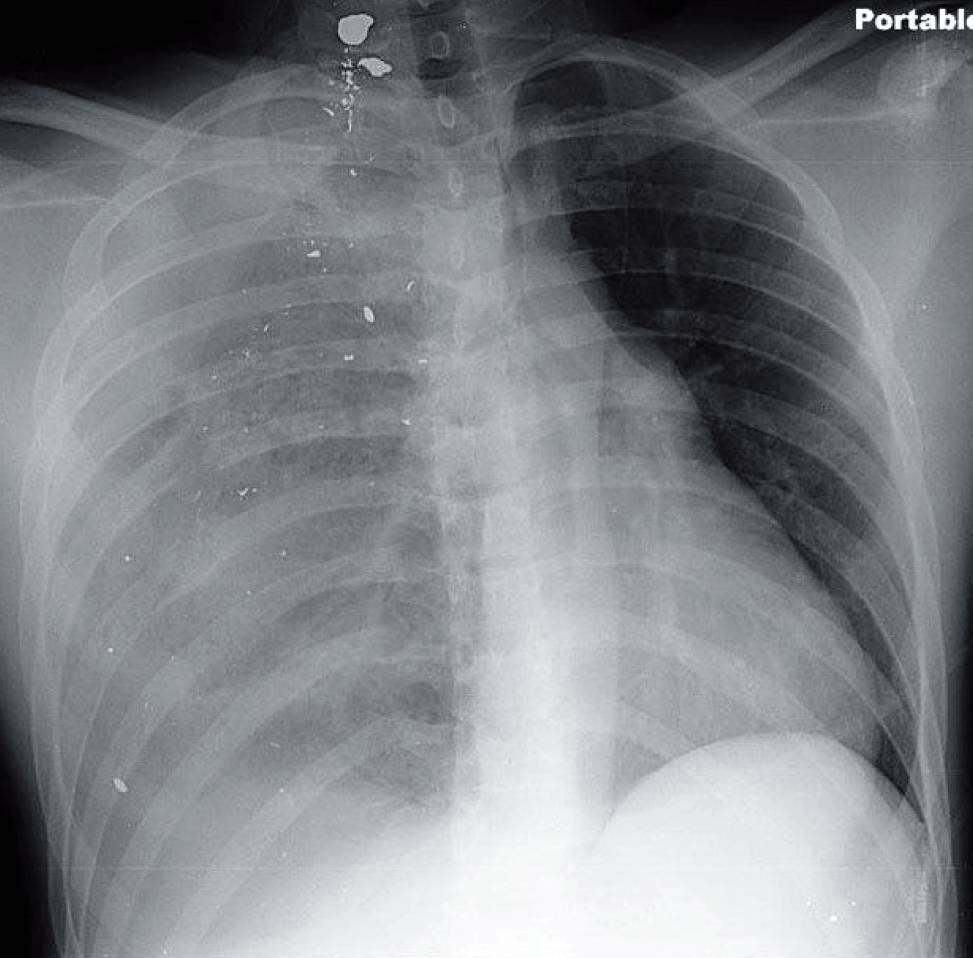
- Single-view portable radiograph shows multiple bullet fragments on the right with shift of the heart and mediastinum leftward. Pulmonary contusions and lacerations are seen near the bullet fragments.
- Increased opacification is seen in the right apex and increased lucency in the right base.
Differential Diagnosis
Although the tension component may prompt one to consider pneumothorax, the density of the pleura is somewhat mixed. The combination of pleural densities is indicative of either a tension hydropneumothorax or a tension hemopneumothorax.
Teaching Points
- Hemopneumothorax usually follows trauma and can result in tension physiology. Penetrating trauma is more likely to result in a tension hemopneumothorax than blunt trauma.
- The radiographic appearance can be confusing because the presence of blood increases the attenuation of the pleural space.
- When supine, the fluid should collect in the more dependent location (apex) while the gas component will rise in the least dependent portion (base).
Management
- Tension hemopneumothorax requires emergent drainage.
- Further imaging is performed after thoracostomy tube drainage. The quantity and rate of drainage will help determine management. If the initial drainage is a large volume of blood or the rate of drainage is brisk, thoracotomy may be indicated.
READ MORE: Penetrating Chest Trauma Algorithm
Further Reading
Shanmuganathan K, Matsumoto J. Imaging of penetrating chest trauma. Radiol Clin North Am. 2006 Mar; 44(2): 225 – 238.
