
This post is an answer to the Case – Patient with Myasthenia Gravis and Hypoxia
Findings
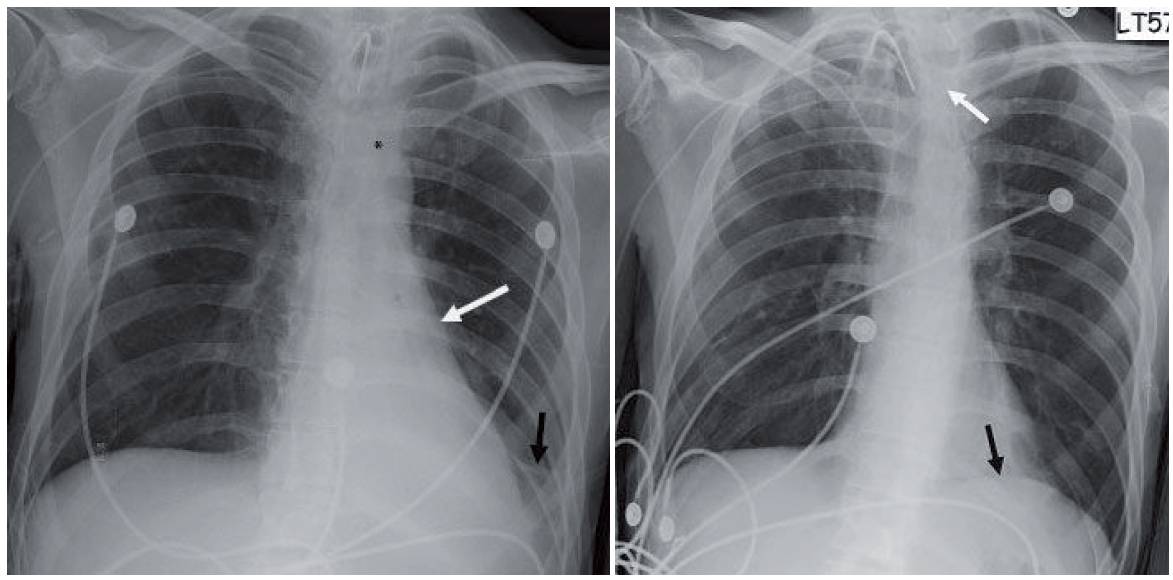
- Initial chest radiograph (first image) shows a retrocardiac opacity with air bronchograms and narrowed distances between the left ribs. The left hemidiaphragm cannot be seen behind the heart and the left heart border appears straightened. Also note the inferior location of the left hilum.
- Follow-up chest radiograph obtained the following day shows near-complete resolution. The left hemidiaphragm can now be seen (black arrow in second image) and the left heart border has regained the normal curvature. The peripherally inserted catheter flipped into the left brachiocephalic vein (white arrow).
Differential Diagnosis
Left lower lobe collapse and pneumonia are the two main considerations. The volume loss strongly supports the former.
Teaching Points
- Left lower lobe collapse assumes the shape of a left retrocardiac triangle. The base of the triangle will obscure the left hemidiaphragm.
- The aerated upper lobe will allow the left heart border to be visible. The volume loss results in left ward rotation of the heart. The net result is an altered appearance to the cardiac silhouette more akin to a right anterior oblique projection.
- The altered left heart border appears straighter than normal. This finding has been referred to as the flat waist sign (white arrow in first image).
- Lingular linear atelectasis is another finding in left lower lobe collapse (Nordentsrom’s sign). This comes from the altered orientation of the lingular bronchi with hyperexpansion (black arrow in first image).
- Two other findings of left lower lobe collapse include shift of the anterior junction line and the top of the knob sign. In the latter, shifted mediastinal soft tissues obscure the top of the aortic arch (asterisk in first image).
Management
With simple collapse, management rests on pulmonary toilet and occasional bronchoscopy to clear the mucus. If no prior studies are available, the collapse should be followed to resolution to exclude a central mass.
SIMILAR CASE: 25-year-old Woman with Abrupt Decrease in Oxygen Saturations
Further Reading
- Gurney JW. Atypical manifestations of pulmonary atelectasis. J Thorac Imaging. 1996 Summer;11(3):165-75. PMID: 8784730.
- Woodring JH, Reed JC. Radiographic manifestations of lobar atelectasis. J Thorac Imaging. 1996 Spring;11(2):109-44. doi: 10.1097/00005382-199621000-00003. PMID: 8820022.