This post is an answer to the Case – Woman with a History of a Mitochondrial Myopathy
Findings
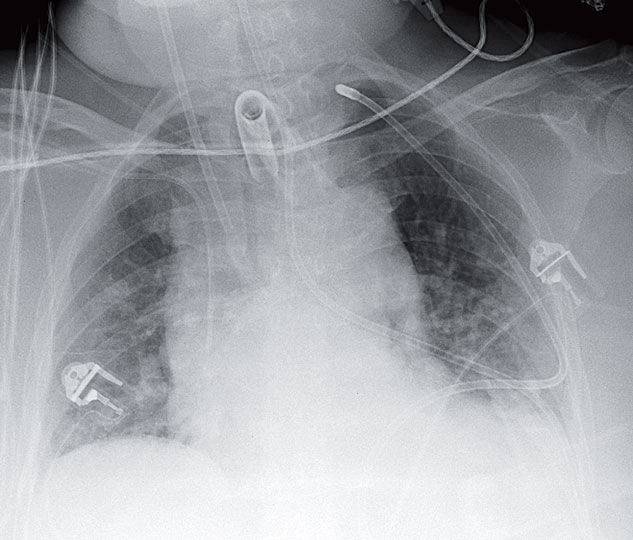
Portable radiograph from the intensive care unit (ICU) shows a tracheostomy and right subclavian central line in usual position. The nasogastric tube, however, is not in the expected location. It can be seen entering the left mainstem bronchus and exiting the anteromedial basal segment into the pleural space, eventually ending up in the apex of the left hemithorax.
Differential Diagnosis
There should be no differential diagnosis for the misplaced nasogastric tube.
Teaching Points
- Complications from misplaced feeding tubes are easily detected by chest radiography.
- Pleuropulmonary complications represent the most common complications after coiled feeding tubes in the pharynx/hypopharynx and placement in the distal esophagus. They result from inadvertent passage of tubes in the tracheobronchial tree with eventual perforation into the lung and pleural space.
- Because of the orientation of the bronchi, right bronchial placement is more common than left .
- Traditional clinical criteria of proper tube placement, including insufflation of air with sounds auscultated in the region of the stomach; aspiration of gastric fluid; and absence of cough, have been shown to be unreliable in ICU patients.
Management
Obviously, a misplaced nasogastric tube should not be used for feeding. It should be removed. When communicating the finding to the ICU team, a follow-up radiograph should be suggested as these misplaced catheters may result in pneumothorax.
SIMILAR CASE: A 92-year-old Woman with Nasogastric Tube for Feeding
Further Reading
- Bankier, A., Wiesmayr, M., Henk, C. et al. Radiographic detection of intrabronchial malpositions of nasogastric tubes and subsequent complications in intensive care unit patients. Intensive Care Med 23, 406–410 (1997). https://doi.org/10.1007/s001340050348
- Lo JO, Wu V, Reh D, Nadig S, Wax MK. Diagnosis and Management of a Misplaced Nasogastric Tube Into the Pulmonary Pleura. Arch Otolaryngol Head Neck Surg. 2008;134(5):547–550. doi:10.1001/archotol.134.5.547