This article is an answer to the Case – A 40-year-old Man with Cough and Dyspnoea
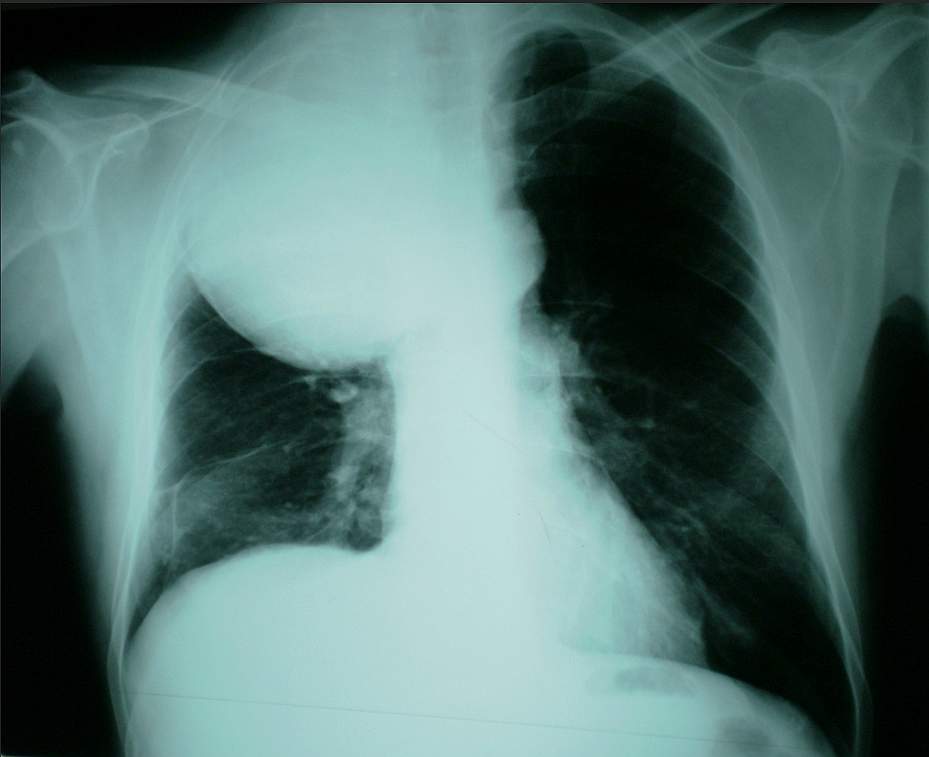
On the chest radiograph, a large sharply marginated mass with uniform opacity was demonstrated projected over the right upper lung. CT and MR imaging was recommended for confirming the localization of the mass to either the lung or the pleura and for more details of the tumour appearance.
CT images showed a well-circumscribed homogeneously non-enhancing lung lesion without associated involvement of bone and without calcification.
MRI provided superior demonstration. T1- and T2-wighted images showed a well-circumscribed mass without evidence of spiculation or satellite nodules. A peripheral rim of enhancement in the lesion was demonstrated after the administration of gadolinium.

Differential diagnosis included bronchogenic carcinoma, various metastatic lesions, mesothelioma, lymphoma, Wegener’s granulomatosis, pyogenic abscess, intrapulmonary haematoma, rheumatoid nodules, histoplasmosis, and coccidiomycosis.
A fine needle guided biopsy (FNB) was performed. The histological and immunochemical (Ki-67 pos.>60%, vimentin, CD99, Bcl-2, CK7, EMA, CK19 positive) examination confirmed the diagnosis of PPSS.