
This blog post is an answer to the Case – 23-Year-Old Man Involved in Motor Vehicle Accident
CT scan findings
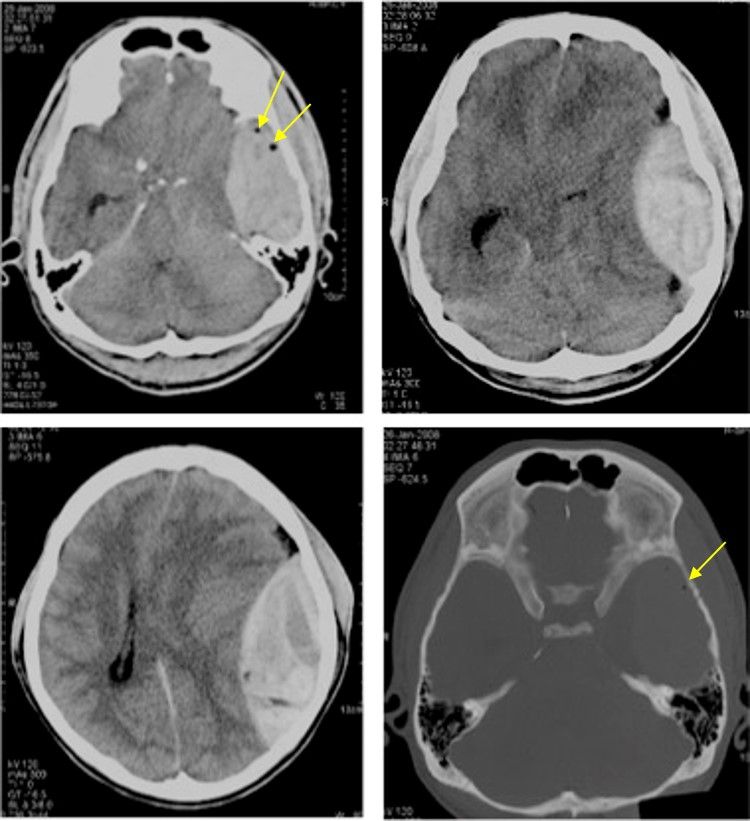
- Axial non-contrasted CT scan of the brain with soft tissue and bone window shows a lens-shaped hyperdensity in the left cerebral convexity. It does not cross the suture.
- An area of isodense to the brain parenchyma is seen within this hyperdense region that represent active hemorrhage (swirl sign).
- Air pockets are also seen within this hyperdense area (arrows).
- There is compression of the underlying brain parenchyma with effacement of the cerebral sulci.
- Subfalcine and uncal herniations are seen.
- There is significant midline shift to the right side. The ipsilateral lateral ventricle is compressed and there is minimal dilatation of the temporal horn of contralateral lateral ventricle.
- There is non-displaced fracture of left temporal bone with adjacent scalp hematoma.
Discussion
Traumatic extradural hemorrhage occurs in 3-4% of trauma cases. CT appearance is described as well-defined biconvex or lentiform-shaped hyperdense extra-axial mass. It is most common in temporal and parietal region. It can cross the midline, can extend above and below the tentorium cerebelli but does not cross cranial sutures.It is associated with skull fracture in 85-95% of cases.
Signs suggestive of poor prognosis in EDH include:
- presence of swirls sign
- significant midline shift of more than 5mm
- presence of traumatic subarachnoid hemorrhage
- obliteration of basal cisterns and hematoma thickness of more than 15mm or hematoma volume of more than 30cm3
Pneumocephalus is the presence of air in the cranial vault. The majority of cases are due to either trauma (75-90%) or surgery. Only 0.5% to 1% of all episodes of head trauma result in pneumocephalus.
Traumatic pneumocephalus occurs with air entering the epidural space as a result of basal skull fracture comes from the sinuses in the floor of the anterior or middle cranial fossa, or the orbit. If the dura is breached, air will reach the subdural space; this occurs in about 28% of cases of pneumocephalus. Tearing of the arachnoid will allow air to enter the subarachnoid space. Distinction of subdural and subarachnoid air can be difficult if the two coexist.CT scan is extremely sensitive, and can identify as little as 0.5 cc of air in the intracranial spaces.
Similar Cases: