A 48-year-old man was referred to the emergency department for chest trauma related to a motorcycle accident. The findings on cardiac auscultation and electrocardiography were consistent with possible dextrocardia.


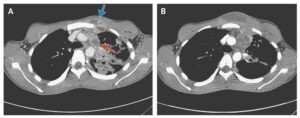
A chest radiograph and computed tomographic (CT) scan showed a 90-degree rightward rotation of the cardiac silhouette (Fig 1, Panel A, arrow) and great vessels (Fig 1, Panel C, arrows), with left tension pneumothorax and multiple rib fractures (Fig 2, Picture 1), bilateral pulmonary contusion (Fig 2, Pictures 1 and 3), and ruptured spleen.
A total-body CT scan showed rightward rotation of the pulmonary artery and aorta (Fig 1, Panel C), rotation of both atria (Fig 2, Picture 1), and rotation of both ventricles (Fig 2, Picture 3). The mediastinal shift that was caused by the tension pneumothorax (Fig 2, Picture 5) caused mild circulatory instability (blood pressure, 80/40 mm Hg; heart rate, 115 beats per minute; and oxygen saturation as measured by pulse oximetry, 92% while breathing 6 liters of supplemental oxygen) without neurologic impairment.
The patient underwent emergency spleen removal and left pleural drainage. A one-way-valve effect contributed to the tension pneumothorax, with progressive buildup of air within the pleural space that pushed the mediastinum to the opposite hemithorax, obstructing venous return to the heart and leading to circulatory instability.
A total of 24 hours after pleural drainage, the patient’s heart moved leftward, back into its original position (Fig 1, Panel B, arrow), with complete anatomical and physiological recovery of the great vessels (Fig 1, Panel D, arrows) and other areas (Fig 2, Pictures 2, 4, and 6).
A follow-up echocardiogram and CT scan did not show the presence of any relevant anatomical disruption of the heart, vessel tears, heart-valve dysfunction, or impairment of cardiac contractility caused by the previous rotation of the heart.
- MORE Similar Cases with Pneumothorax: