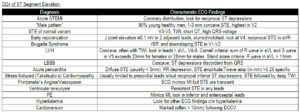
An acute inferior myocardial infarction (IMI) typically causes ST-segment elevation (STE) in leads II, III, and aVF on the 12-lead electrocardiogram (ECG). In addition to these findings, an inferior myocardial infarction (IMI) can also produce ST-segment depression (STD) or T-wave inversion (TWI) in lead I and aVL.
In fact, STD or a new TWI in lead aVL is often the first ECG abnormality seen in patients with an acute inferior myocardial infarction. This underscores the importance of obtaining serial ECGs in patients with a suspected acute coronary syndrome.
When an acute inferior myocardial infarction is diagnosed, a right-sided ECG should be obtained to exclude the presence of a concomitant right ventricular myocardial infarction (RVMI). RVMIs can complicate 30% to 50% of acute IMIs.
A right-sided ECG is performed by taking leads V3 through V6 and placing them on the right side of the chest. These leads are then labeled V3R through V6R. STE of 0.5 mm or greater in one or more of leads V4R through V6R has a sensitivity of 90% and specificity of 91% for an RVMI.
In an RVMI, STE is more commonly seen in lead V4R compared with leads V5R and V6R. In fact, STE greater than 1 mm in lead V4R suggests a proximal occlusion of the right coronary artery (RCA) and an increased risk for atrioventricular block.
Additional ECG findings that suggest an RVMI include:
- STE in lead V1
- STE in lead III that is greater than the STE in lead II
- isoelectric ST segment in lead V1 with STD in lead V2
It is important to diagnose an RVMI because it affects patient management. Patients with an acute myocardial infarction commonly receive nitrate medications in addition to other time-sensitive therapies.
Patients with an RVMI are preload dependent and require intravenous fluids to maintain adequate perfusion. A precipitous decline in blood pressure can occur when nitrates are administered to patients with an RVMI. Any medication that may decrease preload should be avoided in the setting of an RVMI.
Morphine has been shown to increase infarct size and decrease coronary blood flow by up to 13% in patients with an RVMI. Morphine should be avoided in patients with an RVMI. Additional therapies for patients with an RVMI remain the same as those for patients with non-RVMIs.
Key Points
- RVMI can complicate up to 50% of IMIs.
- When an IMI is identified, a right-sided ECG should be obtained.
- STE in lead V4R indicates a proximal occlusion of the RCA and an increased risk for AVB.
- STE in lead V1 with concomitant depression in lead V2 suggests an RVMI.
- Patients with an RVMI are preload dependent. Avoid nitrates and administer intravenous fluids.
Suggested Readings
- Chhapra D, Mahajan SK, Thorat ST. A study of the clinical profile of right ventricular infarction in context to inferior wall myocardial infarction in a tertiary care centre. J Cardiovasc Dis Res. 2013;4:170–176. https://pubmed.ncbi.nlm.nih.gov/24396256/
- Inohara T, Kohsaka S, Fukuda K, Menon V. The challenges in the management of right ventricular infarction. Eur Heart J Acute Cardiovasc Care. 2013;2:226–234. https://academic.oup.com/ehjacc/article/2/3/226/5921795?login=true
- Ondrus T, Kanovsky J, Novotny T, et al. Right ventricular myocardial infarction: From pathophysiology to prognosis. Exp Clin Cardiol. 2013;18:27–30. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3716484/
- Waldo SW, Brenner DA, Li S, et al. Reperfusion times and in-hospital outcomes among patients with an isolated posterior myocardial infarction: insights from the National Cardiovascular Data Registry (NCDR). Am Heart J. 2014;167(3):350–354. https://pubmed.ncbi.nlm.nih.gov/24576519/
- Wei EY, Hira RS, Huang HD, et al. Pitfalls in diagnosing ST elevation among patients with acute myocardial infarction. J Electrocardiol. 2013;46:653–659. https://www.sciencedirect.com/science/article/abs/pii/S0022073613003415