Swallowed foreign body impaction occurs most commonly in children and edentulous or otherwise impaired adults.
- In adults, by far and away the most common foreign body ingestion is a meat bolus impacting a preexisting anatomic structure.
- In children, the most common foreign body ingestion are coins.
While most of these ingestions will pass spontaneously, nearly 20% will require endoscopy and 1% will require surgical removal.
Symptoms of Ingested Foreign Body
The manifestations are surprisingly broad and include the typical presentation of:
- dysphagia and
- neck tenderness after eating
But can also include:
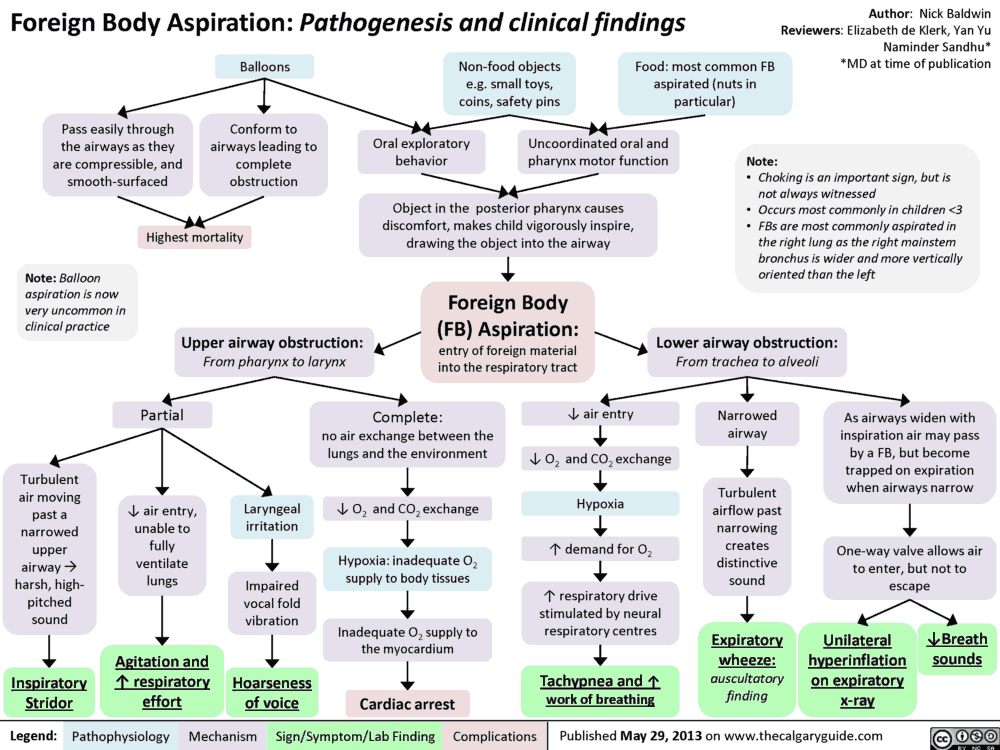
- choking
- wheezing
- respiratory distress
- or even a relatively asymptomatic patient
To make matters worse, this is a patient population that quite often is not able to provide an accurate history.
Common Sites for Foreign Body Impaction
The esophagus naturally narrows at three places:
- the upper esophageal sphincter
- the aortic arch
- the diaphragm
All of these sites are common areas for impaction; however, many impactions, particularly recurrent ones, are secondary to webs, strictures, or masses.
While an acute presentation is more common, partially obstructing lesions can present in a delayed fashion (days later) and are at higher risk for esophageal perforation.
Diagnosing Foreign Body Ingestions
The clinical history is not always sufficient. These patients are often elderly, are very young, or have a psychiatric diagnosis that would make their clinical history less reliable.
In the vast majority of cases, a screening radiograph is appropriate. Be aware that many foreign bodies are not radiopaque! These include fish bones, most pills, and meat boluses. Therefore, a negative radiograph does not exclude a foreign body. In fact, approximately two-thirds of ingestions are radiopaque.
There are a few tricks to reading these plain films that may be helpful:
- Disk batteries often appear to be a double shadow or coin stack.
- Tracheal foreign bodies are typically best seen on lateral projection.
- Esophageal foreign bodies are better seen in a coronal view.
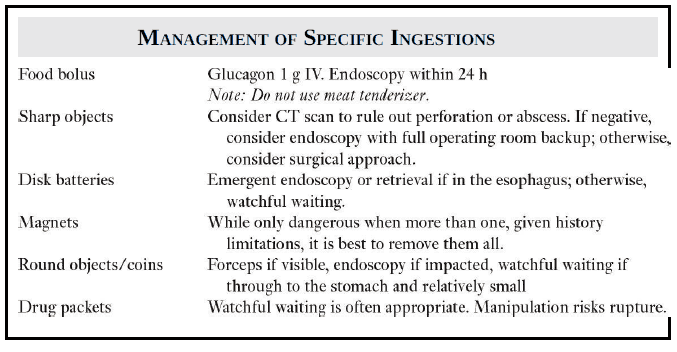
Managing Foreign Body Ingestions
The timing of intervention will vary depending on the clinical scenario, even with similar ingested objects (image). The emergency medicine mantra of “the ABCs” still reigns here, and as with any other case, airway compromise is a true emergency.
Other “hard signs” for emergent endoscopy include:
- inability to handle secretions
- fever
- crepitus
- free air on radiograph
- if the object is sharp, a disk battery, or a magnet
Cases to consider urgent endoscopy (rather than emergent) include:
- large objects
- inability to tolerate oral solids or liquids
- foreign bodies in the esophagus longer than 24 hours
Special Consideration in Foreign Body Ingestions in Pediatric Patients
Special consideration should be given to pediatric patients. Their ingestions are often more insidious, and the history from caregivers is paramount.
A plain film is usually very helpful in these cases; however, avoid oral contrast as it does not add much information and runs a high risk of aspiration.
Once the ingested foreign object has been localized and identified, as long as it is not acutely dangerous, the child can be discharged and followed with serial imaging from his or her pediatrician until passage.
Follow-up is recommended for anyone who has presented with this complaint, as a thorough evaluation for the cause of the impaction will help prevent recurrence and possibly other complications.
In some cases, the episode will lead to the unmasking of another more sinister diagnosis, such as a malignancy, that requires prompt intervention. Ultimately, the goal is to prevent perforation, which runs a considerable mortality risk, both acutely and in the future.
Key Points
- Assess the airway first
- Localization and identification of the foreign object will guide treatment
- Disk batteries, magnets, and sharp objects usually require immediate intervention
- Get follow-up for these patients
References / Suggested Readings
- Ikenberry SO, Jue TL, Anderson MA, et al. Management of ingested foreign bodies and food impactions. Gastrointest Endosc. 2011;73(6):1085.
- Khan MA, Hameed A, Choudhry AJ. Management of foreign bodies in the esophagus. J Coll Physicians Surg Pak. 2004;14:218.
- Kramer RE, Lerner DG, Lin T, et al. Management of ingested foreign bodies in children: A clinical report of the NASPGHAN Endoscopy Committee. J Pediatr Gastroenterol Nutr. 2015;60:562.