This post is an answer to the ECG Case 230
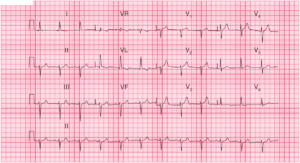
- Rate: 72 bpm
- Rhythm:
- Regular
- Sinus rhythm
- Axis: Normal
- Intervals:
- PR – Normal (120ms)
- QRS – Normal (80-100ms)
- QT – 360ms (QTc Bazette 380-400 ms)
- Segments:
- ST Elevation in leads V1 (0.5mm), V2 (1.5mm), V3 (1mm), V4 (0.5mm), aVL (subtle)
- ST Depression in leads II, III, aVF
- Additional:
- Biphasic (up-down) T waves in leads V2, V3
- T wave inversion in leads I, V4-6
- Q waves in leads I, II, III, aVF, V2-6
What happened next ?
No old ECG’s available. ECG performed by GP ~1 hour earlier showed identical changes to above ECG, serial ECGs within the ECG showed no dynamic change, and interestingly the ECG post intervention remained the same as above.
Urgent cardiology review was arranged given ECG features and on-going pain. The patient was given aspirin, ticagrelor, heparin, opiates, GTN and was taken for urgent angiography which showed:
- LMCA – normal
- Prox LAD – irregularities
- Mid LAD – 90% lesion TIMI II distal flow –> PCI
- Cx – irregularities
- RCA – irregularities
Post angio ECHO showed:
- Regional wall motion abnormalities infero-antero-septal regions
- EF 50%
- Normal valvular function
Troponin peaked at 11 (normal <0.05) and the patient was discharge after an uneventful in-patient recovery.
Interpretation
I think this one is tricky and as you can see above was associated with a mid-LAD lesion. Given the precordial Q waves, on-going chest pain, and high biomarker rise we can’t say this is a true Wellen’s pattern, although at a brief glance the T wave changes are the most striking ECG feature. Given the 3 days of preceding pain I wonder how ‘acute’ this ECG is, especially given the non-dynamic changes.
READ MORE: ECG Interpretation – All you need to know
SIMILAR CASES: