This post is an answer to the Case – Child with Dyspnea and Episodes of Syncope
CXR findings
- The cardiac apex is rounded and elevated off the left hemidiaphragm (suggestive of right ventricular hypertrophy)
- The pulmonary bay is concave
- There is pulmonary oligaemia
- No evidence of cardiac failure
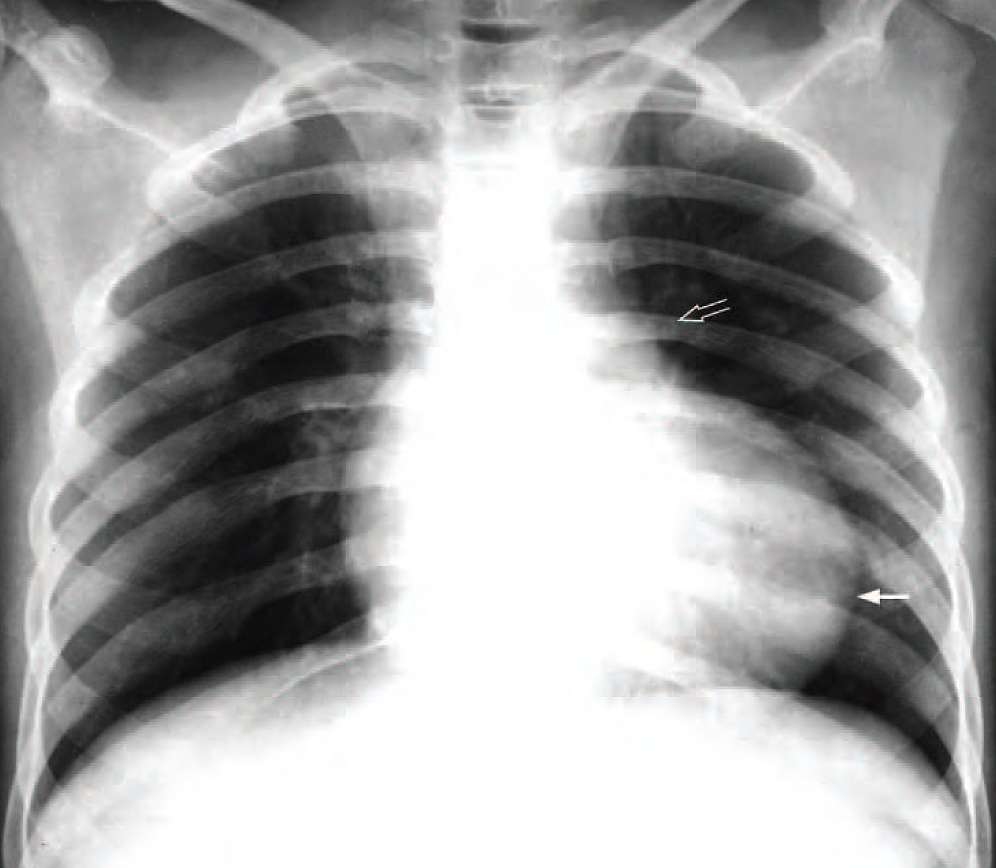
Diagnosis: Tetralogy of Fallot.
Chest radiograph of a cyanosed child showing a rounded and elevated cardiac apex (arrow) suggestive of right ventricular hypertrophy, a concave pulmonary bay (open arrow) and pulmonary oligaemia
Discussion
Tetralogy of Fallot accounts for approximately 8% of all congenital heart disease and is the most common CHD with cyanosis in a child after one year of age. The condition is characterised by:
- Obstruction to the pulmonary outflow tract usually by pulmonary infundibulum stenosis – occasionally by pulmonary valvular stenosis.
- Right ventricular hypertrophy resulting from the pulmonary outflow tract obstruction
- Ventricular septal defect
- An overriding aorta – the aorta overrides the interventricular septum
Pathophysiology
In fetal life, the pulmonary circulation is filled in a retrograde fashion via the ductus arteriosus and thus RV hypertrophy does not develop. After birth, with closure of the ductus arteriosus, a R to L shunt develops via the VSD, resulting in cyanosis. Pressure overload and RV hypertrophy subsequently develop secondary to the pulmonary infundibulum stenosis.
Tetralogy of Fallot may be associated with other anomalies, the commonest being left pulmonary artery stenosis (40%), bicuspid pulmonary valve (40%) and right sided aortic arch (25%).
Treatment is primarily surgical. Palliative operations such as the Blalock-Taussig shunt – which involves end-to-end anastomosis of the subclavian artery to the pulmonary artery opposite the aortic arch – may be performed.
The presence of a boot shaped heart in a child with cyanosis and heart murmur should raise the suspicion of tetralogy of Fallot.