This post is an answer to the ECG Case 316
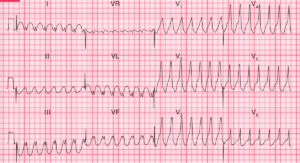
- Bradycardia, rate ~42bpm
- Irregular rhythm
- Atrial activity visible but unrelated to QRS complexes
- 2 distinct QRS morphologies
- Complexes #1,2,4,5,7
- Complexes #3,6
- Marked QRS Prolongation
- Massive T waves in leads I, aVF, V4-6
- Deep T wave inversion in leads V1-3
Interpretation
Looking at the ECG in isolation the major life-threatening concern for these features would be hyperkalemia. This would be consistent with the patient’s history of renal disease secondary to SLE. Contributing factors could also be severe acid/base disturbance, again consistent with renal failure.
Given known cardiac SLE involvement it is possible the patients baseline ECG may have QRS prolongation and longstanding ST / T wave changes.
What happened next?
An urgent blood gas was performed which showed a potassium of 9.2 mmol/L and pH 7.1. The patient was also acutely fluid overloaded which caused her dyspnea.
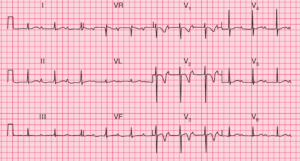
Following initial treatment of salbutamol nebuliser, iv calcium gluconate, iv dextrose / insulin and sodium bicarb, there was significant improvement in the ECG. The patient’s potassium was now 8.6 mmol/L with no change in pH. She was taken for urgent dialysis.
READ MORE: Disorders of Potassium Homeostasis (Hypokalemia and Hyperkalemia)
SIMILAR CASES: