
The rhythm in is regular at a rate of 130 bpm. The QRS complex duration is increased (0.22 sec) and the axis is extremely leftward, between –30° and –90° (positive QRS complex in lead I and negative QRS complex in leads II and aVF).
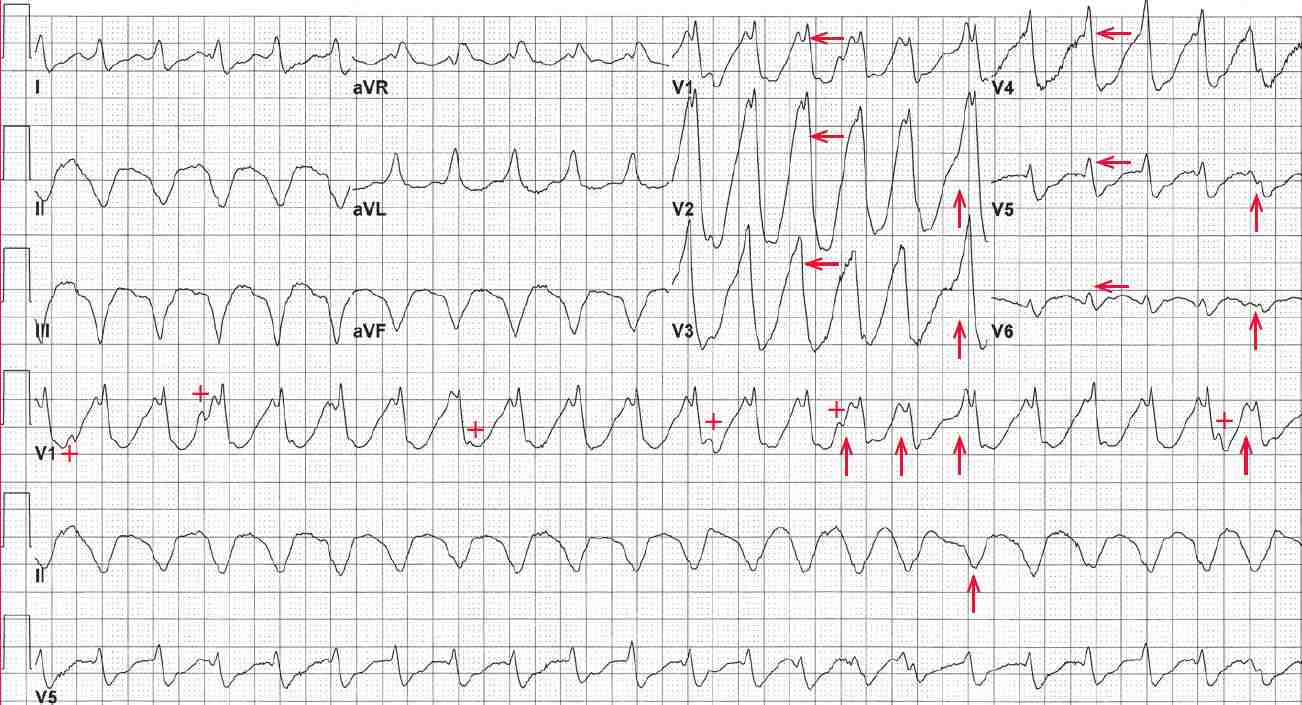
Although no distinct atrial activity is seen, some variable waveforms (+) are present, best seen in the lead V1 rhythm strip between the 1st and 2nd QRS complexes, before the 4th QRS complex, between the 12th and 13th QRS complexes, between the 14th and 15th QRS complexes, and between the last two QRS complexes. These are superimposed P waves that are dissociated from the QRS complexes.
In addition, there are subtle changes in QRS morphology (↑). The morphology of the QRS complexes is not typical for either right or left bundle branch block. In addition, there is positive QRS complex concordance across the precordium, with tall R waves from lead V1 through V5 and possibly V6.
These features (AV dissociation, changes in QRS complex and ST-T wave morphology, QRS complex width > 160 msec, positive concordance of QRS complexes across the precordium) support a diagnosis of sustained ventricular tachycardia.
The changes in the QRS complex and ST-T wave morphology are due to the fact that ventricular activation is not via the normal His-Purkinje system but rather is by direct myocardial activation. This may result in changes in the sequence or direction of myocardial activation.
In contrast, any sinus, atrial or junctional rhythm is conducted to the ventricle through the same pathway (ie, AV node His-Purkinje system) and, therefore, all the QRS complexes and ST-T waves are uniform.
Positive QRS concordance is also seen only when there is direct myocardial activation, such as with a ventricular complex, a preexcited QRS complex (Wolff-Parkinson-White) or a paced complex.

![Read more about the article Conduction Blocks at the AV Node (AV Blocks) [With Examples]](https://manualofmedicine.com/wp-content/uploads/2021/05/Excerpt-AV-Blocks-300x243.jpg)