This article is an answer to the ECG Case 157
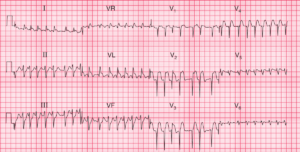
There is a regular rhythm at a rate of 84 bpm. There is a P wave (*) in front of each QRS complex, with a stable PR interval (0.18 sec). The P wave is upright in leads I, II, aVF, and V4-V6 and negative in lead aVR. The P-wave morphology is normal. This is a normal sinus rhythm.

The QRS complex duration is normal (0.08 sec), and there is a small R′ in lead V1 (↓), indicating delayed activation of the right ventricle.
The T waves (+) in leads II, III, and aVF are tall and hyperacute (T-wave upstroke and downstroke are equal) in contrast to the normal T wave, which is asymmetric (ie, the upstroke of the T wave is slower than the downstroke). T waves that are tall, peaked and, most importantly, symmetric (hyperacute) are seen with hyperkalemia. Hyperkalemia may be systemic or localized, as is seen in acute transmural myocardial infarction (MI).
Hyperacute T waves are the first abnormality noted in an acute transmural MI as a result of localized hyperkalemia. They occur in the area of myocardium involved and are seen even before there are any ST-segment changes. Hence this is a very early acute inferior wall MI.
Also noted are ST-segment depressions in leads V2-V4 (^), which possibly represent involvement of the posterior wall. This can be confirmed by recording from posterior leads placed on the back below the left scapula (leads V7-V8). These ST-segment depressions may also represent reciprocal ST-segment changes (ie, the same ST-segment changes [elevations] viewed from another angle or direction). However, the ST segments in leads II, III, and aVF are not yet elevated, so these are probably not reciprocal ST-segment changes.