This article is an answer to the ECG Case 177
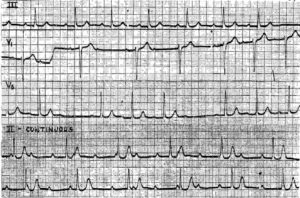
The ECG shows the rhythm is irregularly irregular as there is no pattern to the RR intervals seen. The average heart rate is 144 bpm. The QRS complex duration is normal (0.10 sec) and the axis is extremely leftward between –30° and –90° (positive in lead I and negative in leads II and aVF). As the QRS complexes in leads II and aVF have an rS morphology, this is a left anterior fascicular block.

Noted are Q waves in leads I and aVL (↑), consistent with an old lateral wall myocardial infarction. There are prominent R waves in V1 (←), and poor R wave progression from leads V3–V6. In V5–V6, the S wave is deep (→) with an R/S ratio < 1. These features suggest right ventricular hypertrophy.
There are only three arrhythmias associated with an irregularly irregular rhythm. This includes sinus arrhythmia (one P-wave morphology and a stable PR interval); multifocal atrial tachycardia (rate > 100 bpm), or multifocal atrial rhythm or wandering atrial pacemaker (rate < 100 bpm) (> 3 different P-wave morphologies with no P-wave morphology being dominant and variable PR intervals); and atrial fibrillation (no organized P waves).
In this ECG, there are P waves (+) seen before each QRS complex with variable or nonconsistent PR intervals (└┘). In addition, the P-wave morphology is variable, with > 3 different morphologies seen. These features (irregularly irregular rhythm at a rate > 100, variable P-wave morphologies and variable PR intervals) are the features of a multifocal atrial tachycardia.
Multifocal atrial tachycardia is most commonly associated with pulmonary disease, especially if there is pulmonary artery hypertension with elevated right atrial and right ventricular pressures. It may also be seen with severe left ventricular dysfunction and heart failure due to any cause, ie, valvular, cardiomyopathy, or coronary disease.
As the mechanism for this arrhythmia is multiple ectopic foci, this arrhythmia cannot be terminated with cardioversion. Therapy is primarily directed at rate control by blocking the AV node, and the most effective agents are beta-blockers or a calcium-channel blocker, especially verapamil. Although data are poor, there is some suggestion that therapy with magnesium and/or potassium may be beneficial.
READ MORE:
- ECG Changes in Chronic Obstructive Pulmonary Disease (COPD)
- Do not confuse Multifocal Atrial Tachycardia with Atrial Fibrillation
SIMILAR CASES: