This post is an answer to the ECG Case 183
The ECG shows a regular rhythm at a rate of 260 bpm. There are no distinct P waves noted. The QRS complex duration is increased (0.12 sec) and there is a right bundle branch block morphology with a broad R wave in V1 (←) and broad S waves in leads I and V5–V6 (→).
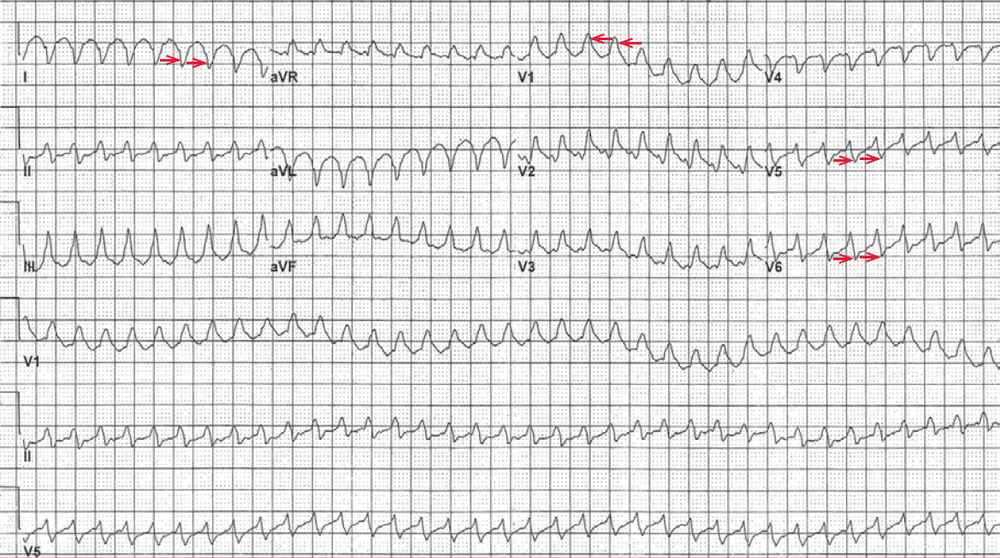
In addition there is a rightward axis between +90° and +180° (negative QRS complex in leads I and positive QRS complex in lead aVF). This is suggestive of a left posterior fascicular block, although an old lateral wall myocardial infarction is suggested by the possible QS complex morphology in leads I and aVL.
This rhythm may be either atrial flutter with 1:1 AV conduction or ventricular tachycardia, which at this rate is often referred to as ventricular flutter. In addition, there is low QRS voltage (< 5 mm or little boxes in each limb lead and < 10 mm in each precordial lead).
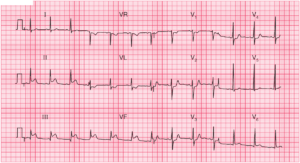
The next ECG (see below) made shortly after the first shows evidence of atrial activity in leads I I, I I I, aVF, and V1–V3 (+). The atrial waveforms are undulating without any isoelectric baseline between them. The atrial rate is 260 bpm and hence this is atrial flutter with 2:1 AV conduction.

The atrial rate is identical to the ventricular rate seen in the first ECG, and hence the rhythm is indeed atrial flutter with 1:1 conduction. An important concept is “same rate same rhythm.” A right bundle branch block morphology is not seen on the second ECG, indicating that the first ECG had a rate-related right bundle branch block.
Atrial flutter with 1:1 conduction is not common and generally reflects the presence of high sympathetic tone or elevated catecholamine levels that enhance AV nodal conduction. Situations in which this occurs include hyperthyroidism, post exercise, severe infection/ sepsis, heart failure, and pulmonary embolism.
When the QRS complex is narrow, this diagnosis is easier to establish, as any regular narrow complex tachycardia at a rate > 260 is atrial flutter with 1:1 conduction. When the QRS complex is wide, the arrhythmia may be either supraven tricular with a rate-related or preexistent bundle or it may be ventricular tachycardia. It may be difficult to distinguish between these two arrhythmias.
READ MORE: Atrial Flutter – ECG Interpretation [With Examples]
SIMILAR CASES: