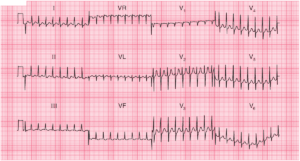
This post is an answer to the ECG Case 212
- Rate: Mean ventricular rate 78 bpm
- Rhythm:
- Complex rhythm
- Alternating broad & narrow QRS complexes
- Complexes #4,6,8,10
- Sinus
- Narrow Complex ~70ms
- Complexes #1,3,5,7,9,11,13
- Premature ventricular complexes (PVC)
- Broad complexes (~140ms)
- Complex #2
- Preceded by abnormal p wave
- PR interval very short (~70ms)
- Premature junctional complex (PJC)
- Axis:
- Sinus complexes – Inferior (~90 deg)
- Ventricular complexes – LAD (-65 deg)
- Intervals:
- Sinus complexes (#4,6,8,10)
- PR – Normal (~125 ms)
- QRS – Normal (70-80 ms)
- QT – 480 ms
- Ventricular complexes (#4,6,8,10)
- QRS – Broad (140 ms)
- QT – 360 ms
- Complex # 2
- PR – Short (~70ms)
- QRS – Normal (70-80 ms)
- QT – 380 ms
- Sinus complexes (#4,6,8,10)
- Segments:
- ST Elevation – Sinus Complexes
- Leads V1 (0.5mm) V2 (2.5mm) V3 (6mm) V4 (3mm)
- ST Depression – Sinus Complexes
- Leads II, III
- Note ST elevation evident in PVC’s in leads aVL,V2, V3
- ST Elevation – Sinus Complexes
- Additional:
- Variable morphology ventricular complexes
- #7 & #9 Notching QRS
- Regular relationship between narrow complex and broad complex
- R-R interval 500ms
- Partial RBBB morphology in narrow QRS complexes
- Variable morphology ventricular complexes
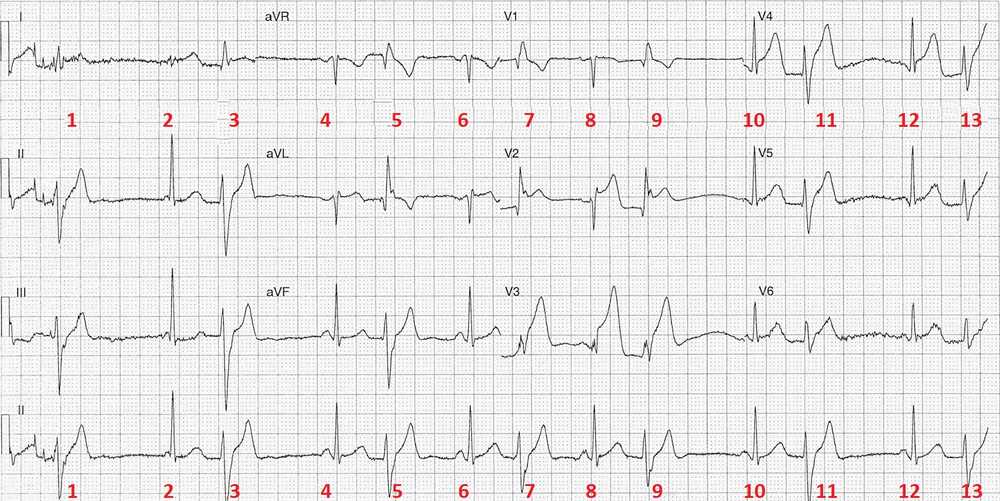
Interpretation
Acute Anterior STEMI with regular PVC’s and a single PJC.
Clinical Outcome
The ST segment changes were immediately recognised and the patient was transferred for urgent angiogram and PCI. His angiogram showed:
- LM – no stenosis
- LAD – occluded mid – PCI
- Cx – no stenosis
- RCA – dominant no stenosis
- Left ventriculogram – Ejection fraction 55%
READ MORE