This post is an answer to the ECG Case 214
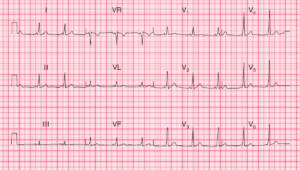
- Rate: 66 bpm
- Rhythm: Regular, Sinus rhythm
- Axis: Borderline LAD (~ -30 deg)
- Intervals:
- PR – Normal (~180ms)
- QRS – Normal (80ms)
- QT – 400ms (QTc Bazette ~ 420 ms)
- Segments:
- Minor ST depression lead III
- Additional:
- T wave inversion in leads II, III, aVF, V4, V5, V6
- Biphasic T wave in leads aVR, V3
- Early precordial transition between V1 and V2
- Dominant R wave in V2
- Prominent T wave in lead V2
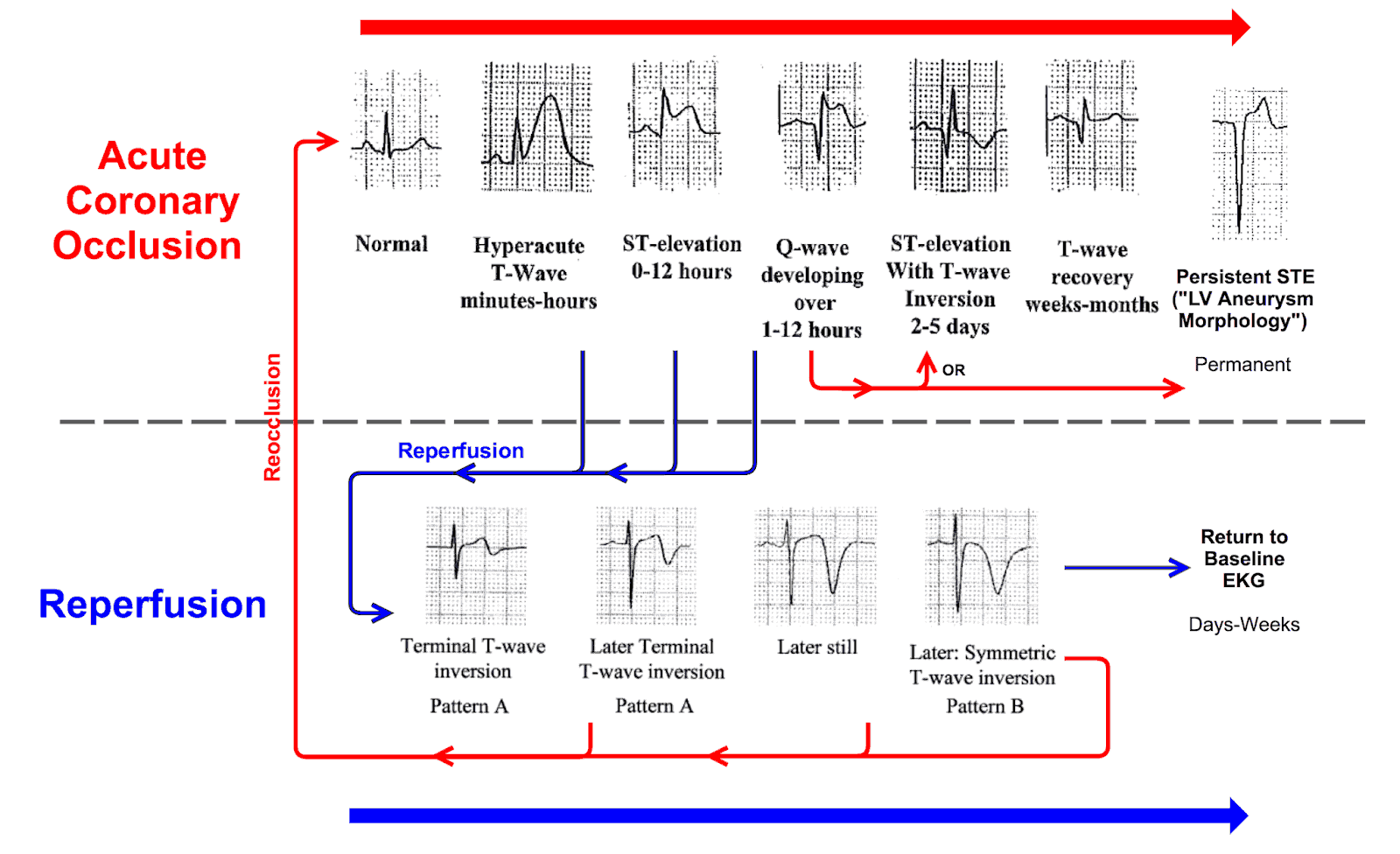
Interpretation
The ECG shows ischemia with re-perfusion (deep T wave inversion).
What happened next ?
The patient was immediately discussed with cardiology services. Treated with aspirin, clopidogrel, and placed on a heparin infusion and admitted to CCU. The patient remained pain free, troponin peaked at 12 hours, 4.8 (normal <0.05), and the patient was transfer the next day for angiography. The angio showed:
- Right coronary: 98% stenosis –> stented
- Circumflex: 80% stenosis
- Left anterior descending: 80% proximal stenosis
- Left main: 20% proximal stenosis
- Left ventricle: Inferior hypokinesis with normal LV function
SIMILAR CASES