This post is an answer to the ECG Case 216
- Rate: 78 bpm
- Rhythm: Regular
- Axis: Normal ( 40 deg)
- Intervals:
- PR – Normal (~140ms)
- QRS – Normal (80ms)
- QT – 400ms (QTc Bazette ~ 450 ms)
- Segments:
- Up-sloping ST Elevation in lead V1-4 (1mm)
- Subtle ST Depression in Lead II
- Additional:
- Voltage Criteria LVH
- Q waves in Leads II, III, aVF, V4-V6
- Biphasic T waves in V1-4
- Positive to negative deflection
- T Inversion in Lead III
- Notched P wave in Leads II, III
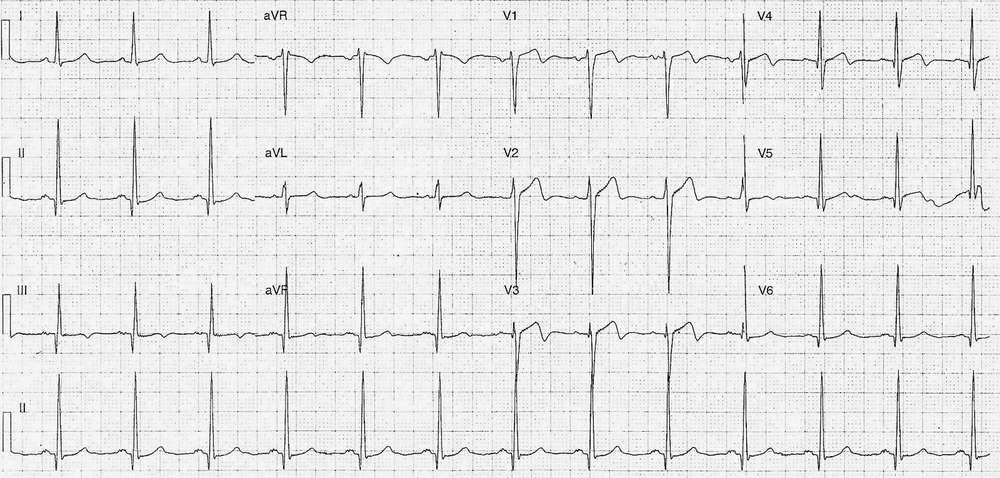
Interpretation
Given clinical history of chest pain and T wave morphology, the ECG is suggestive of Wellens’ Syndrome (type 2).
Wellens’ Syndrome represents critcal LAD disease with a mean time to infarction of approximately 8 days. ECG features of Wellens’ are:
- Type 1 Pattern – deep symmetrically inverted T waves in leads V2 & V3
- Type 2 Pattern – positive to negative biphasic T waves in leads V2 & V3
With:
- No pathological precordial q waves and no loss of R wave progression
- Patient with history of chest pain
Note:
- Typical Wellens’ ECG features usually occur on the painfree ECG
- T wave changes may extend into the lateral precordial leads.
- Patients may have normal biomarkers.
- Exercise stress testing may precipitate acute infarction and should be avoided
What Happened Next ?
The patient gave a history strongly suggestive of cardiac chest pain and was discussed with the cardiology team. Following initial treatment with aspirin, clopidogrel, heparin, the patient was transferred to another facility for ongoing management.
His initial troponin I result was elevated at 2.3 mcg/L [normal <0.05] and the patient underwent angiography and PCI that day. His angiography showed:
- LAD – Critical proximal stenosis which was stented
- LCx – moderated mild disease
- RCA – moderate proximal disease
- LV – global hypokinesia
READ MORE: