This post is an answer to the ECG Case 246
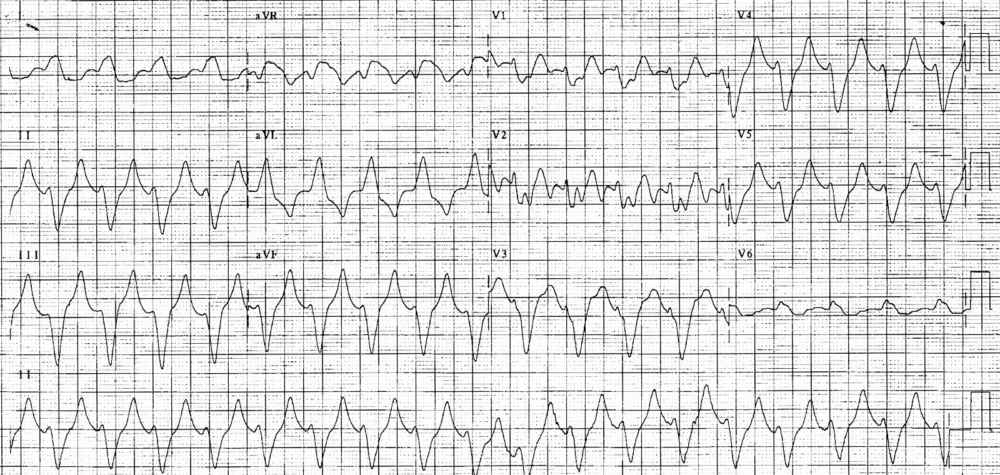
- Rate: ~108 bpm
- Rhythm:
- Regular
- Likely sinus tachycardia
- Axis: LAD
- Intervals:
- QRS – Prolonged (200ms)
- QT – 440ms
- Segments:
- ST elevation in leads II, aVF, aVR, V3
- ST depression in leads I, aVL, V1, V6
- Additional:
- Prominent T waves in leads II, III, aVF, aVL, V4-5
- No fusion / capture beats
- Absence of concordance
Interpretation
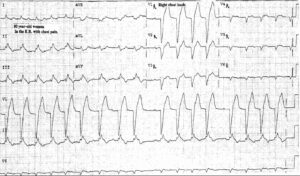
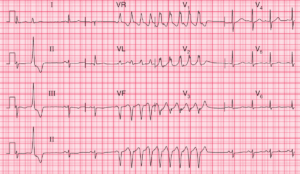
Wide complex tachycardia.
The general differentials for WCT include:
- VT
- SVT with BBB / aberrancy / pre-excitation
- Paced rhythms
- Toxins e.g. sodium channel toxicity
- Do not forget Hyperkalaemia
The extent of the widening plus the clinical stem of young patient with a metabolic disorder strongly suggests hyperkalaemia as the cause, and that’s exactly what the labs showed.
SIMILAR CASES: