ECG Interpretation
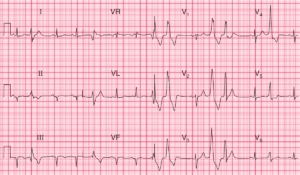
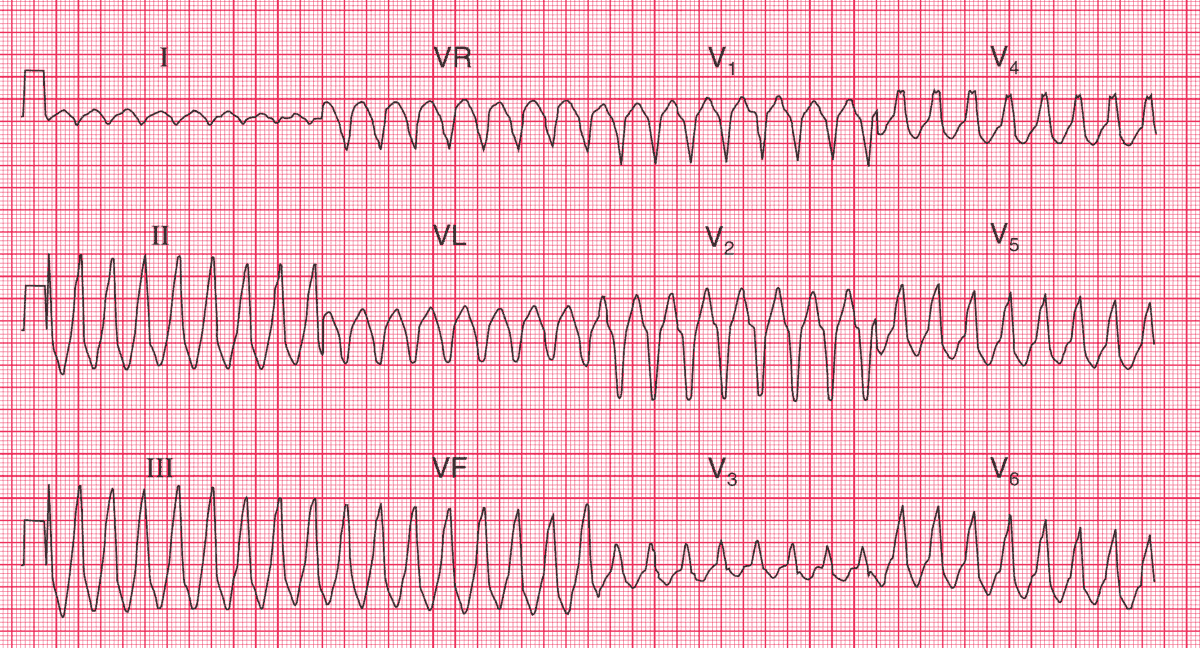
- Broad complex tachycardia at 200/min
- No P waves visible
- Right axis deviation
- QRS complex duration 200 ms
- QRS complexes show no concordance
- Left bundle branch block (LBBB) pattern
Clinical Interpretation
A broad complex tachycardia like this is probably of ventricular origin. In this case, features against the rhythm being ventricular tachycardia are the right axis deviation and the lack of concordance in the QRS complexes (i.e. the complexes point downwards in leads V1–V2 and upwards in the other chest leads).
The combination of right axis deviation and an LBBB pattern in a broad complex tachycardia suggests that the origin is in the right ventricular outflow tract.
What to do ?
Any patient with an arrhythmia and evidence of haemodynamic compromise (in this case, breathlessness and a very low blood pressure) needs immediate cardioversion. While preparations are being made, it would be reasonable to try intravenous lidocaine or amiodarone.
Once the arrhythmia has been corrected, an electrophysiological study is needed, because right ventricular outflow tract tachycardia is the one variety of ventricular tachycardia that should be amenable to ablation therapy.
- READ MORE:
- Similar Cases:
- ECG Case 78: Ventricular tachycardia in a 60-year-old man
- Ventricular Tachycardia with Retrograde 4:3 Wenckebach Conduction
- Ventricular Tachycardia from Cocaine Overdose
- Ventricular Tachycardia in 69 year-old man
- Idiopathic Posterior Fascicular Ventricular Tachycardia (VT)
- Hypokalemia that led to Ventricular Tachycardia (Torsades de pointes)