This post is an answer to the ECG Case 262
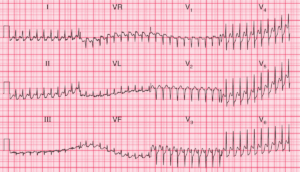
- Rate: 72 bpm
- Rhythm: Regular, Sinus rhythm
- Axis: Normal
- Intervals:
- PR – Short (~100ms)
- QRS – Pronlonged (110ms)
- QT – 340ms
- Segments:
- ST Depression in lead aVL, V6
- ST Elevation in leads aVR, V1 (<1mm)
- Additional:
- Delta wave best seen in leads I, V2, V3
- Notching initial portion QRS leads II, V4-6
- Marked prominent T wave in lead V3
- Q waves in leads III, aVF
Interpretation
- Wolff-Parkinson- White
- Short PR, delta waves and QRS widening
- Right Lateral Wall AP using Arruda Algorithm
- Inferior Q waves secondary to AP conduction – “pseudo-infarction”
- Prominent T wave in lead V3
- This looked suspicious to me and would have prompted serial ECG’s and urgent review of any prior ECGs
What happened next ?
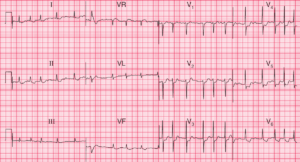
The patient had known WPW at the time of presentation and had a normal stress echo and EST the year prior following an Emergency Department attendance with chest pain.
Old ECG’s were identical to the one shown here and serial ECG’s revealed no dynamic changes. Serial biomarkers were negative and the patient was discharge with out-patient cardiology follow-up.
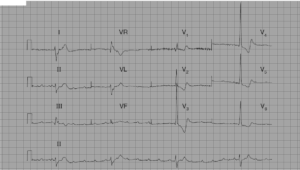
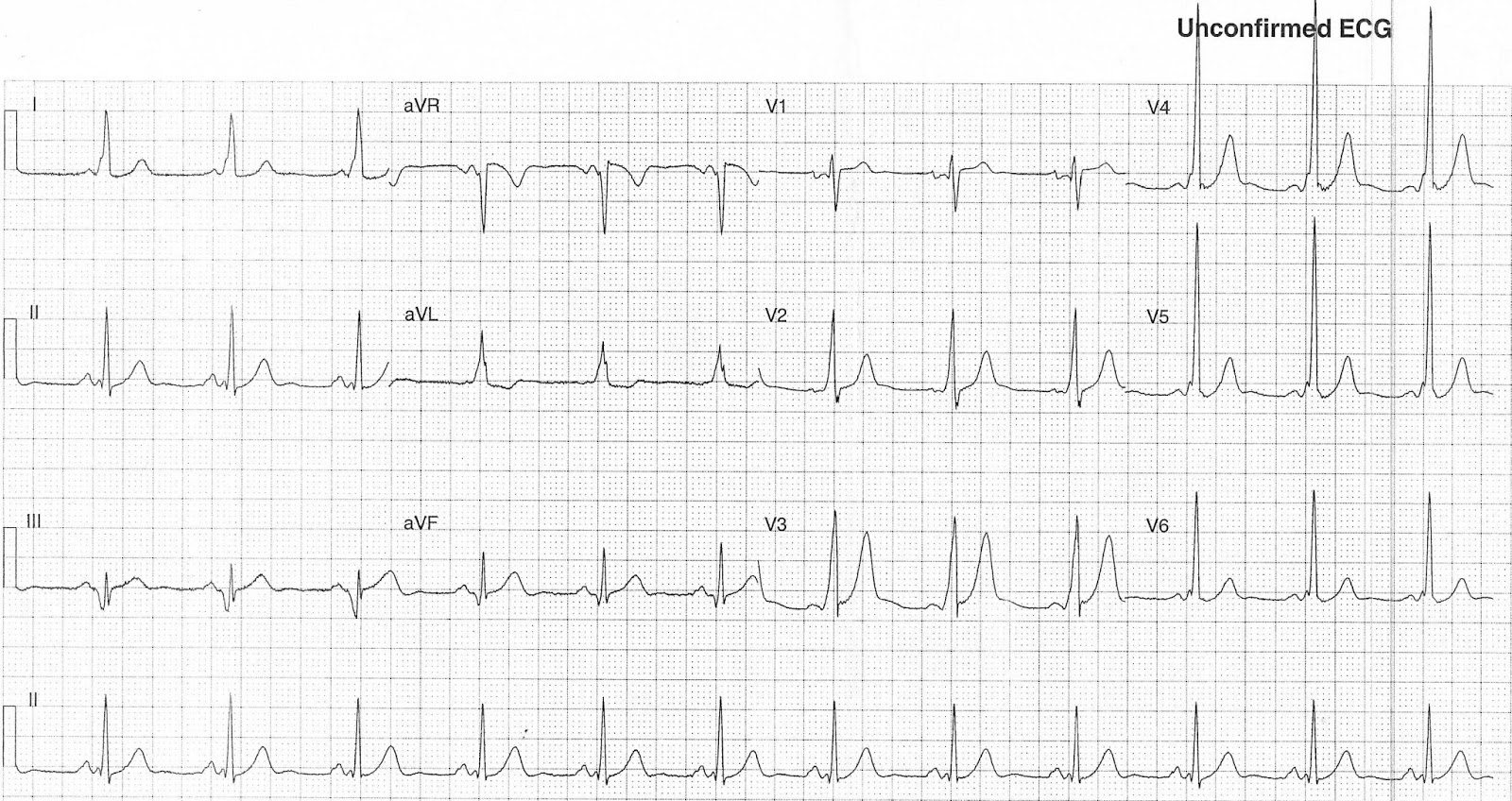
SIMILAR CASES: