
This post is an answer to the Case – Sudden Loss of Consciousness and Left-Sided Weakness
What is seen on the CT ?
- Wedge-shaped low attenuation lesion involving the right frontal and parietal lobe in the right middle cerebral artery (MCA) territory.
- Hyperdense line running through the low attenuation area along the course of the branches of the right MCA (dense MCA sign).
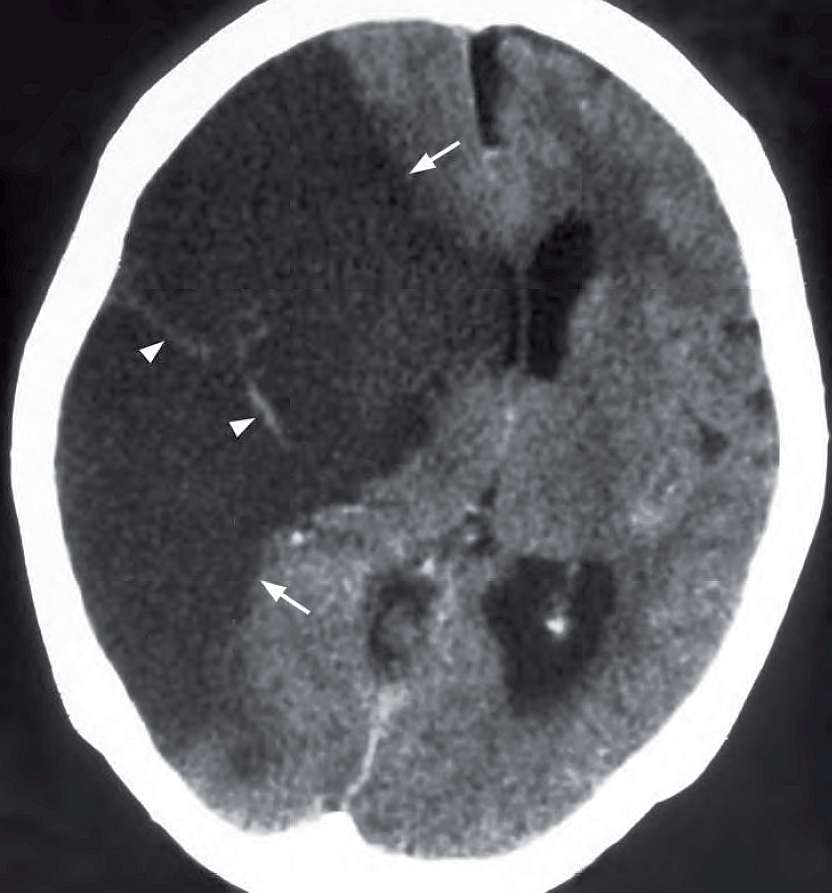
Non-contrast axial CT scan shows a wedge shaped area of low attenuation (arrows), with effacement of underlying cortical sulci, involving both grey and white matter in the right MCA territory. Also note the mass effect on the ventricles and contralateral shift.
The diagnosis is an acute right MCA territory infarct. The arrowheads show a hyperdense thrombus in the branches of the right MCA.
Cerebral Infarction – Discussion
Cerebral infarction is the irreversible loss of brain tissues due to ischaemia or haemorrhage.
Role of imaging:
- To confirm the clinical diagnosis
- To identify any intracranial haemorrhage
- To detect other lesions which may clinically mimic an infarct, e.g. tumour, vascular malformation, subdural haematoma
- To detect early complications such as subfalcine/transtentorial herniation and haemorrhagic transformation
CT is the initial imaging of choice for acute stroke. However, it may not demonstrate a cerebral infarct during the first 12 hours. At this time its role is to rule out the presence of intracranial haemorrhage as this defines the treatment options.
An infarct may be treated by anticoagulants/ thrombolytics whereas these are contraindicated in the presence of an intracranial haemorrhage.
Early signs of cerebral infarction on CT:
- Loss of grey-white matter interface
- Sulcal effacement
- Hyperdense clot within thrombosed artery (dense MCA sign)
Luxury perfusion (seen on contrast CT): represents hyperaemia in an ischaemic area; the increased perfusion is due to compensatory vasodilatation due to parenchymal lactic acidosis
Subacute infarcts on CT:
- Grey-white matter oedema
- Gyral enhancement on contrast CT
- Haemorrhagic component seen in up to 40%
Chronic infarcts on CT :
- Parenchymal tissue loss
- Cystic encephalomalacia
In the presence of occlusion of the main ICA a large area of infarct/oedema will be seen involving multiple vascular territories in the cerebral hemisphere with mass effect and contralateral shift of midline structures. Structures supplied by the posterior circulation through the vertebral arteries are unaffected as these vessels remain patent.
Ischaemic areas limited to the posterior circulation should raise the suspicion of vertebral artery dissection which may be due to minor trauma, twisting/hyperextension of the neck.
READ MORE: Stroke and TIA – From Diagnosis to Treatment

