
This post is an answer to the Case – Patient with Chronic Headache, Unsteadiness and Frequent Falls
What is shown on the CT ?
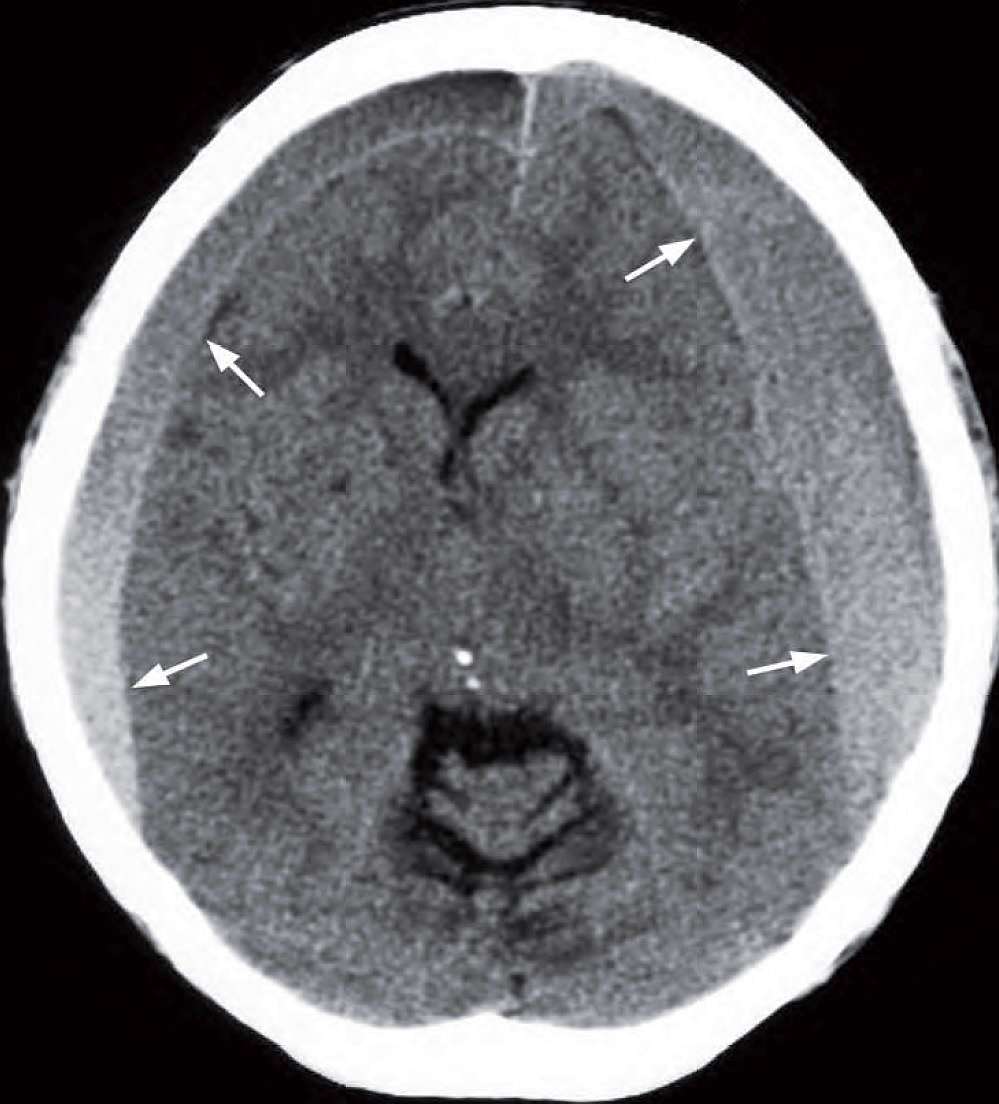
- Crescentic bilateral subdural collections isodense/slightly hyperdense to brain.
- Both the frontal/anterior horns of the lateral ventricles are compressed.
- Mild midline shift to the right.
Diagnosis
Non-contrast axial CT of the brain shows bilateral subdural haematomas (arrows) that are acute/subacute.
Discussion
Subdural haematomas (SDH) are caused by traumatic tear of bridging veins as they traverse the subdural space to dural venous sinuses, which are more vulnerable in elderly patients with atrophic brain and widened subdural space.
Alcoholics and epileptics may develop undetected chronic subdural haematomas as they have repeated falls and the head injuries sustained are trivial and often forgotten (postictal state in epileptics). Also seen in infants in non-accidental injury (NAI).
May enlarge gradually over weeks and months with multiple episodes of small haemorrhages.
Symptoms and physical signs are those of an enlarging intracranial space occupying lesion (SOL) and may be confused with an intracranial tumour until CT reveals the diagnosis.
CT features
- Most are supratentorial in location
- Crescentic in shape and along the surface of the brain
- Unlike extradural haematomas subdural haematomas cross the coronal and lambdoid sutures
- Do not cross dural reflections (falx cerebri, tentorium cerebelli)
- Acute on chronic haemorrhage results in heterogeneous increase in density and rapid increase in size
- There is no consistent relationship to the presence of skull vault fracture
Change of haematoma density on CT with time:
- Acute SDHs are hyperdense to brain or show mixed heterogeneous density
- Subacute SDHs (> 1 week) are isodense and may be difficult to identify – a clue is when the sulci no longer extend all the way to the skull vault. IV contrast may show enhancing membrane and displaced cortical vessels
- Chronic SDHs (> several weeks) are hypodense and may calcify
- Fluid level may be seen in subacute or early chronic SDHs in which the denser debris collects in the dependent portion of the haemorrhage
SIMILAR CASES: