This article is an answer to the Case – Pruritic and Painful Rash
This patient presents with shingles, also known as herpes zoster, which is a reactivation of varicella-zoster virus or human herpesvirus-3.
Herpes zoster often presents first with a prodrome of pruritus, pain or tingling in the dermatome involved, followed by the development of painful grouped vesicles in a dermatomal distribution.
Occasionally, vesicles can involve more than one contiguous dermatome and cross the midline. The most common sites affected are the trunk and face.
‘Hutchinson’s sign’ is the presence of skin lesions in the distribution of the nasociliary branch of nerves, which supplies the nasal tip, dorsum and root of the nose. This is seen with infection of the ophthalmic division of the trigeminal nerve, which is seen in 10%–15% of patients with herpes zoster. It is important to recognize ocular involvement, because ocular scarring and visual loss are potential sequelae.
Ramsay Hunt syndrome is a herpes zoster infection of the geniculate ganglion. In this syndrome, herpes zoster involves the external ear and face and can lead to tinnitus or other auditory symptoms, as well as ipsilateral facial paralysis.
In patients with human immunodeficiency virus (HIV), herpes zoster can manifest with unusual presentations, which include multidermatomal, verrucous and disseminated.
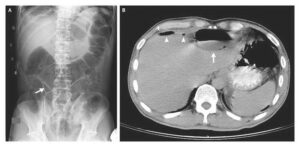
Disseminated herpes zoster, defined as the presence of more than 20 vesicles outside of the area of primary dermatomal involvement or adjacent dermatomes, should lead clinicians to also consider visceral involvement, most commonly hepatic, pulmonary and central nervous system (CNS) infection. Patients who present with these variants should be tested for HIV.
Treatment
Food and Drug Administration (FDA)-approved treatments for herpes zoster include acyclovir, famciclovir and valacyclovir. Treatment should be initiated within 72 hours of the development of skin lesions, although benefit is seen with initiation within 7 days.
Treatment with antiviral medication also reduces the frequency and duration of common sequelae such as postherpetic neuralgia.
Although most cases of herpes zoster resolve without sequelae in children and young adults, postherpetic neuralgia is a common complication in older patients or patients with immune compromise.
Treatment for postherpetic neuralgia includes low-dose tricyclic antidepressants, gabapentin, topical capsaicin, transepidermal nerve stimulation, local analgesics and nerve blocks.