
This article is an answer to the Case – Chest Pain and Dyspnea in 9-year-old Boy
Imaging Findings
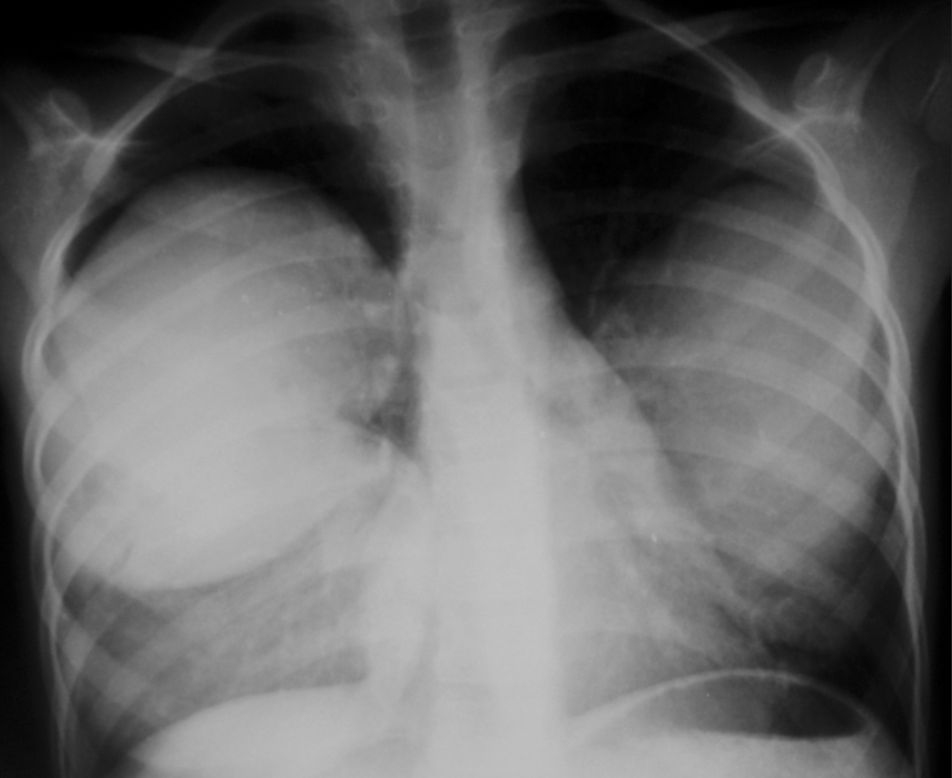
Chest X-ray revealed two nodular opacities (fluid density lesions) in right lung and one in left lung.
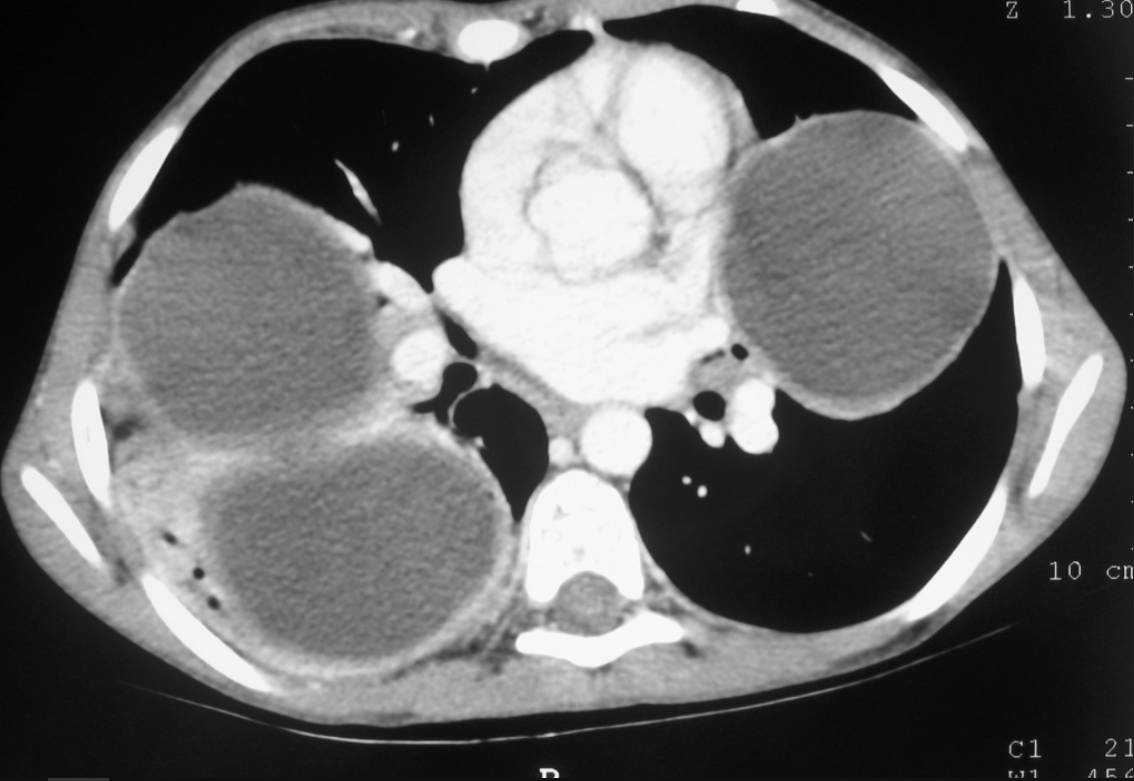
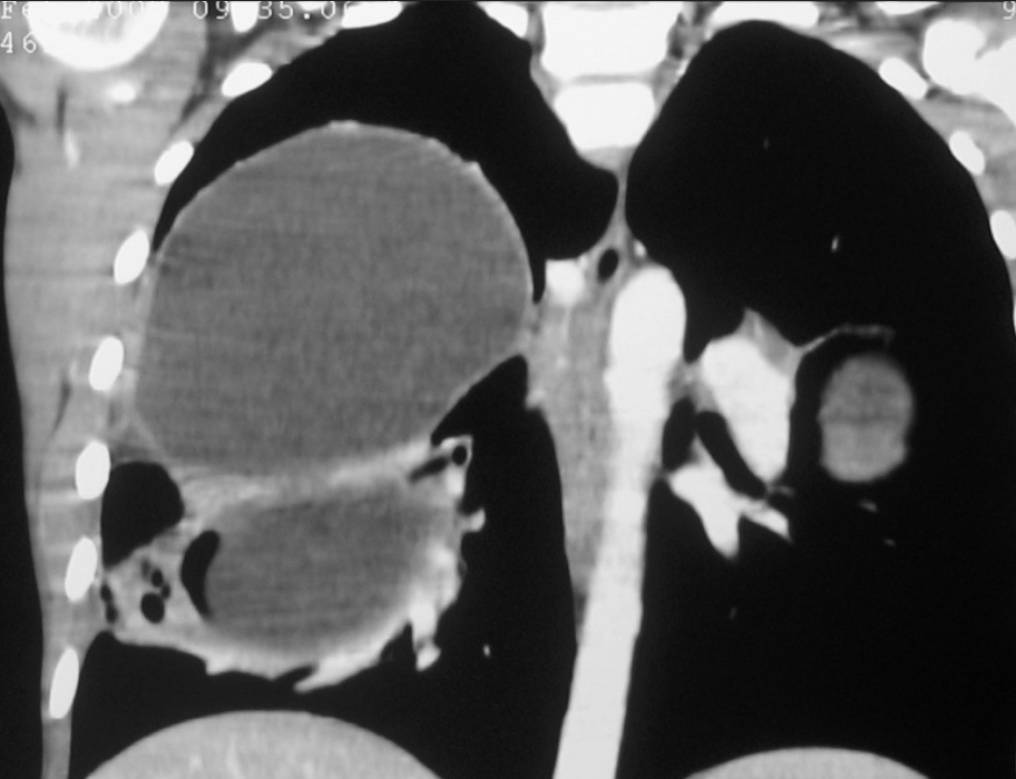
Thorax CT revealed two cysts in right lower and medium lobe of lung and one cyst in lingual lobe of left lung. The diagnosis of hydatid cysts was confirmed at surgery.
Discussion
Hydatid disease (HD) is a worldwide zoonosis produced by the larval stage of the Echinococcus granulosus. The lungs are the second most frequent site of hematogenous spread in adults and probably the most common site in children (15%–25% of cases).
Pulmonary HC have a predilection for the right posterior lung segments, with 60% of cases manifesting in the lower lobes. Bilateral involvement occurs in 20% of cases and multiple cysts in 30% Calcification in pulmonary cysts is very rare (0.7% of cases).
Pulmonary hydatic cysts may vary from 1 to 20 cm in diameter because of their compressibility, the lungs are the only organ in which HC can grow so large. Most cysts are acquired in childhood, remain asymptomatic for a long period of time, and are later diagnosed incidentally at chest radiography.
Imaging appearances and diagnosis of Pulmonary Hydatid Disease
Imaging appearances may vary due to the growth of the parasite and its relationship to adjacent lung tissue. Initially, lung HC generally manifest as type I cysts, being oval or round and having well-defined borders. CT reveals the hypoattenuating nature of these lesions.
Diagnosis is generally easily made in endemic regions on the basis of typical location and imaging findings, but multiple cysts, like our case, can be misdiagnosed as metastases. Daughter cysts (type II) are rarely seen in lung HD.
One of the most common imaging findings in HC is the “meniscus sign,” which occurs when cyst growth produces erosions in the bronchioles that are included in the pericyst; as a result, air is present between the pericyst and the laminated membrane. Some authors consider this to be a sign of impending rupture and an indication for emergency thoracotomy.
Air between the endocyst and pericyst creates the “onion peel sign”. If air continues to enter the cyst cavity, the two layers completely separate from each other. The collapsed and crumpled endocyst floats freely in the most dependent part of the pericyst cavity and produces the “water lily sign”. If the fluid is entirely evacuated by expectoration, the remaining solid components will fall to the most dependent part of the cavity (“mass within a cavity”).
Complications of Pulmonary Hydatid Disease
Complications of lung HC include rupture of the cyst into the parenchyma and pleurall cavity. Bacterial infection of the cyst is the most serious complication commonly seen after rupture (air-fluid level inside the endocyst). The other complication of HC is recurrent acute pulmonary embolism, a rare complication that can be seen when a cyst directly involves the vena cava
SIMILAR CASE: Echinococcal Cysts in the Liver